BASIC INFORMATION
Date & Time: June 4, 2026, 4:14 PM (Indian Standard Time)
Lecture Handout Prepared from the Teaching Session by: Dr. R. K. Mishra
SUMMARY
This lecture provides a comprehensive overview of the use of B-mode ultrasonography to measure the Optic Nerve Sheath Diameter (ONSD) as a non-invasive surrogate for intracranial pressure (ICP) in patients undergoing prolonged laparoscopic or robotic-assisted surgeries. The discussion centers on the physiological changes leading to increased ICP in this surgical setting, including the effects of pneumoperitoneum, hypercapnia, and prolonged steep Trendelenburg positioning. The lecture details the anatomical basis for ONSD measurement, explains the standardized ultrasound technique, and identifies patient populations at higher risk for complications. It critically evaluates reference values and reviews evidence from clinical trials, including a 2026 study from the Brazilian Journal of Anesthesiology on the prophylactic use of mannitol. The session concludes that ONSD ultrasonography is a valuable, dynamic, bedside tool for monitoring trends in ICP, enabling anesthesiologists and surgeons to enhance patient safety by guiding perioperative management, particularly in decisions regarding postoperative care such as delayed extubation.
KEY KNOWLEDGE POINTS
-
Physiological Basis: The optic nerve sheath is a direct extension of the dura mater, and the subarachnoid space surrounding the nerve is contiguous with the intracranial subarachnoid space, allowing changes in ICP to be transmitted and measured.
-
Pathophysiology of Increased ICP: Understanding the combined effects of pneumoperitoneum, hypercapnia, Trendelenburg positioning, and positive end-expiratory pressure (PEEP) on central venous pressure, cerebral blood flow, and cerebrospinal fluid drainage.
-
Standardized Measurement Technique: ONSD should be measured 3 mm posterior to the globe. While there is a discrepancy in the summaries on whether to measure inner-to-inner or outer-to-outer border of the dural sheath, the 3 mm landmark is consistent.
-
High-Risk Patient Populations: Identification of patients with pre-existing conditions (e.g., glaucoma, prior cerebrovascular events, sleep apnea, previous neurosurgery, elderly patients) who are more susceptible to the adverse effects of elevated ICP.
-
Clinical Trial Evidence: A 2026 clinical trial on laparoscopic prostatectomy patients demonstrated that while Trendelenburg position significantly increases ONSD, prophylactic mannitol (0.5 g/kg) did not mitigate this change.
-
Clinical Interpretation: An ONSD greater than 6 mm is a strong indicator of elevated ICP. The evolution of measurements over time (the trend) is often more significant than a single, isolated value, and findings must be correlated with the overall clinical picture.
INTRODUCTION
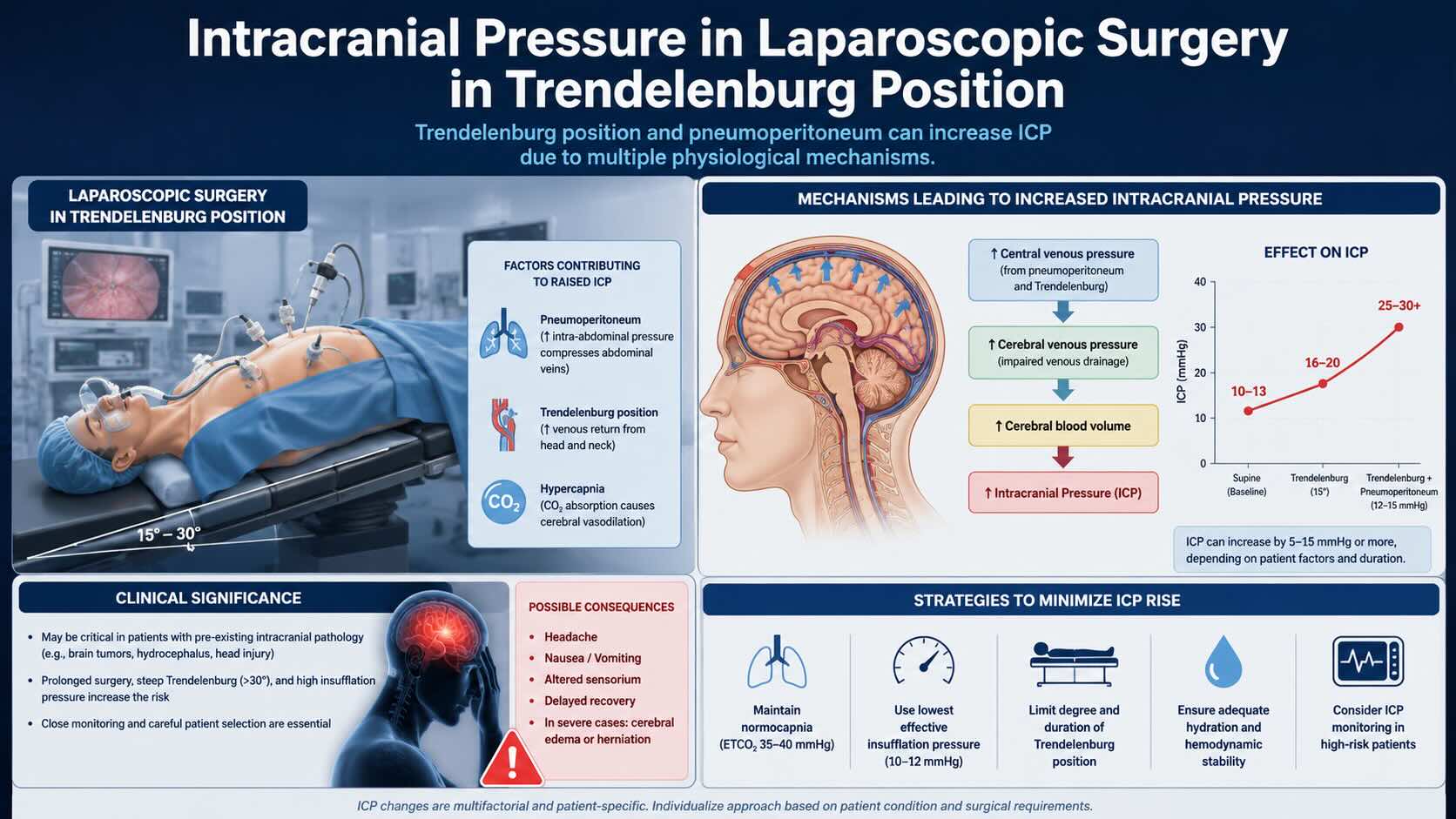
Prolonged laparoscopic and robotic-assisted procedures, particularly in colorectal, urological, and gynecological surgery, frequently require the use of pneumoperitoneum and a steep Trendelenburg position. This combination creates a unique physiological challenge, leading to elevated intracranial pressure (ICP) through increased intra-abdominal pressure, CO2 absorption causing hypercapnia, and gravitational effects impeding venous drainage. While direct, invasive ICP monitoring is not indicated for these procedures, the potential for neurological and ophthalmological complications necessitates a reliable, non-invasive assessment method.
Ultrasonography of the optic nerve sheath diameter (ONSD) has emerged as a valuable tool for this purpose. Because the subarachnoid space surrounding the optic nerve is in direct communication with the intracranial space, changes in ICP lead to corresponding changes in the ONSD. This technique provides anesthesiologists and surgeons with a real-time, indirect measure of intracranial dynamics, serving as a "window to the brain." Understanding and applying this methodology can enhance patient safety, particularly in high-risk populations, and inform perioperative management strategies.
LEARNING OBJECTIVES
-
To describe the physiological mechanisms leading to increased intracranial pressure during laparoscopic surgery in the Trendelenburg position.
-
To explain the anatomical and physiological principles that allow ONSD measurement to serve as a surrogate for ICP.
-
To master the standardized technique for performing ONSD ultrasonography as per current international guidelines.
-
To identify high-risk patient groups, recognize potential clinical consequences of sustained intracranial hypertension, and integrate ONSD findings into perioperative management.
-
To critically appraise the evidence supporting the use of ONSD measurement, including the findings of recent clinical trials regarding prophylactic interventions.
CORE CONTENT
1. Pathophysiology of Intracranial Hypertension in Laparoscopic Surgery
Laparoscopic surgery in the Trendelenburg position creates a multifactorial environment conducive to elevated ICP.
1.1. Effect of Pneumoperitoneum and Patient Positioning
-
Increased Central Venous Pressure (CVP): The insufflated abdomen increases intra-abdominal pressure, which is transmitted to the intrathoracic cavity, elevating CVP.
-
Impaired Cerebral Venous Drainage: The Trendelenburg position, combined with elevated CVP, compromises venous outflow from the brain, leading to central venous and subsequent cerebral congestion.
-
Mechanical Ventilation: The use of positive end-expiratory pressure (PEEP) to maintain oxygenation further increases intrathoracic pressure and exacerbates the impairment of venous return.
1.2. Effect of Hypercapnia
-
Cerebral Vasodilation: Absorption of carbon dioxide from the pneumoperitoneum can lead to systemic hypercapnia. CO2 is a potent cerebral vasodilator.
-
Increased Cerebral Blood Flow (CBF): Vasodilation of cerebral arterioles increases the volume of blood within the fixed cranial vault, contributing significantly to the rise in ICP.
2. Optic Nerve Sheath Ultrasonography: Rationale and Technique
2.1. Anatomical Basis
The optic nerve is an extension of the central nervous system, covered by the pia, arachnoid, and dura mater. The subarachnoid space around the nerve is continuous with the intracranial subarachnoid space. When ICP rises, cerebrospinal fluid (CSF) is forced into this perineural space, causing the elastic dural sheath to expand. This distension is most pronounced approximately 3 mm behind the globe and is measurable via ultrasound.
2.2. Standardized Technique for ONSD Measurement
-
Transducer and Preset Selection: Use a high-frequency (7.5–12 MHz) linear array transducer. If available, select the dedicated "Ocular" or "Ophthalmic" preset, which optimizes gain, depth, and focus.
-
Patient and Probe Preparation: The patient is positioned supine with eyes closed. Apply a generous amount of sterile ultrasound gel over a transparent sterile dressing (e.g., Tegaderm) placed on the closed eyelid to prevent corneal abrasion or infection. The operator’s hand should be rested on the patient’s forehead for stability.
-
Image Acquisition: Gently place the transducer on the dressing over the temporal aspect of the upper eyelid. Adjust depth to visualize the posterior globe, optic nerve head, and retrobulbar optic nerve. The nerve appears as a hypoechoic structure extending posteriorly.
-
Measurement:
-
The measurement must be taken 3 mm posterior to the globe.
-
Freeze the image and use electronic calipers. Two slightly different techniques were described: one measures the internal diameter (inner border to inner border of the hyperechoic dura), while another measures from the outer edge to the outer edge of the hyperechoic sheath. Adherence to a single, consistent institutional protocol is critical.
-
Perform measurements on each eye. A difference of more than 0.5 mm between eyes may indicate an acquisition error and warrants a repeat measurement.
-
3. Indications and Patient Selection
-
Primary Indication: Monitoring patients undergoing prolonged surgical procedures (>2 hours) with anticipated sustained increase in ICP, especially those involving steep Trendelenburg positioning (e.g., robotic pelvic surgery).
-
High-Risk Patient Populations:
-
Patients with Glaucoma (especially closed-angle glaucoma).
-
History of Cerebrovascular Events (e.g., Stroke).
-
Prior Neurosurgery or Brain Injury.
-
Obstructive Sleep Apnea (OSA).
-
Elderly patients with comorbidities (e.g., hypertension, diabetes).
-
-
Exclusion Criteria: Patients with pre-existing ocular pathology (e.g., glaucoma in some study protocols) may be excluded or require preoperative ophthalmological assessment.
4. Reference Values and Interpretation
-
General Reference Values: An ONSD of >5.0 mm is frequently associated with increased ICP. An ONSD greater than 6 mm (e.g., 6.2-6.3 mm) is generally considered a strong indicator of significantly elevated ICP.
-
Population Variation: Baseline ONSD can vary with age and between different ethnic populations.
-
Clinical Correlation: An elevated ONSD is an indicator, not a diagnosis. The trend of serial measurements over time is more clinically significant than a single value. Findings must be correlated with other clinical parameters (e.g., end-tidal CO2, blood pressure) and the patient's overall status.
5. A 2026 Clinical Trial: Mannitol in Laparoscopic Prostatectomy
-
Study Design: A randomized clinical trial published in the Brazilian Journal of Anesthesiology (2026) evaluated 48 patients undergoing laparoscopic prostatectomy. Patients were randomized to receive prophylactic mannitol (0.5 g/kg) or a control.
-
Measurements: ONSD was measured at four time points: after induction (T1), after Trendelenburg positioning (T2), at the end of surgery (T3), and after returning to neutral (T4).
-
Findings: A statistically significant increase in ONSD was observed between the neutral (T1) and Trendelenburg (T2/T3) positions. However, there was no significant difference in ONSD between the mannitol group and the control group at any time point.
-
Conclusion: The study concluded that prophylactic mannitol (at a dose of 0.5 g/kg) did not attenuate the increase in ONSD caused by pneumoperitoneum and the Trendelenburg position in this patient population.
SURGICAL PEARLS
-
Use a Barrier: Never apply the ultrasound transducer or non-sterile gel directly to the eye. Always use a protective transparent film over the closed eyelid.
-
Avoid Globe Compression: Use copious gel and rest your hand on the patient's forehead to avoid applying pressure to the globe, which can cause injury (oculocardiac reflex) and measurement errors.
-
Standardize Your Technique: Adhere strictly to the standardized measurement protocol, especially the 3 mm posterior landmark, to ensure consistent and comparable findings.
-
Interpret with Context: An increased ONSD is an indicator. Correlate the finding with other clinical parameters (EtCO2, blood pressure) to form a complete clinical picture. Focus on the trend over time.
-
Learning Curve: Operator proficiency is crucial and is typically achieved after performing 25-30 scans. It is a relatively simple skill to acquire compared to more complex ultrasound applications.
-
Image Optimization: Adjust gain to clearly differentiate the anechoic nerve/CSF space from the hyperechoic sheath, avoiding "blooming" artifacts from excessive gain.
COMPLICATIONS AND THEIR MANAGEMENT
-
Intraoperative
-
Measurement Risk: The primary risk during measurement is excessive pressure on the ocular globe, which can cause corneal abrasion or an oculocardiac reflex (bradycardia, hypotension). This is managed by immediately releasing pressure.
-
Significant Intracranial Hypertension: If ONSD demonstrates a concerning increase, management strategies may include reducing pneumoperitoneum pressure, correcting hypercapnia by adjusting ventilation, or transiently reducing the degree of Trendelenburg positioning if surgically permissible.
-
-
Early Postoperative
-
Delayed Emergence: An elevated ONSD (>6 mm) in a patient who fails to awaken promptly provides objective data to support a diagnosis of persistent cerebral dysfunction. This justifies conservative management, such as keeping the patient intubated and transferring them to the ICU for continued observation.
-
Postoperative Headache/Agitation: These are common manifestations. Manage symptomatically and rule out other causes.
-
Visual Disturbances: Any new or worsened visual complaint warrants an urgent ophthalmology consultation.
-
-
Late Postoperative
-
Postoperative Cognitive Dysfunction (POCD): While the link is not definitive, minimizing the duration and severity of ICP elevation through intraoperative monitoring may theoretically reduce this risk.
-
MEDICOLEGAL AND PATIENT SELECTION CONSIDERATIONS
-
Informed Consent: For high-risk patients or long procedures, the potential risks associated with prolonged Trendelenburg positioning and pneumoperitoneum (including neurological and visual complications) should be part of the informed consent discussion.
-
High-Risk Patients: Exercise extreme caution in patients with known glaucoma (especially closed-angle), intracranial space-occupying lesions, or recent stroke. The risk-benefit ratio of a laparoscopic versus an open approach should be carefully considered.
-
Role as an Adjunctive Tool: ONSD measurement is a diagnostic aid, not a definitive test. Clinical decisions should not be based solely on this value, but it provides crucial objective data to support clinical judgment.
-
Documentation: Meticulous documentation of preoperative risk factors, intraoperative ONSD findings, the technique used, and postoperative neurological and visual status is essential from a medicolegal standpoint. A documented high ONSD provides strong justification for conservative decisions like delayed extubation.
SUMMARY AND TAKE-HOME MESSAGES
-
Prolonged laparoscopic surgery in the Trendelenburg position predictably increases ICP through venous congestion, hypercapnia, and positional effects.
-
ONSD ultrasonography is a validated, non-invasive, real-time method to indirectly assess changes in ICP, serving as a vital monitoring tool.
-
Adherence to a standardized technique, particularly measuring 3 mm posterior to the globe, is crucial for obtaining accurate, reproducible, and clinically relevant data.
-
An ONSD >6 mm is a strong indicator of elevated ICP. In a patient with delayed emergence, this finding supports continued intubation and ICU admission.
-
Prophylactic mannitol was not found to prevent the ONSD increase associated with pneumoperitoneum and Trendelenburg positioning in a recent clinical trial.
-
Special attention must be paid to high-risk patients, and ONSD findings must always be interpreted within the complete clinical context.
MULTIPLE CHOICE QUESTIONS (MCQs)
-
Which of the following is the primary mechanism by which pneumoperitoneum increases intracranial pressure (ICP)?
a) Direct transmission of pressure through the diaphragm
b) Increased cerebral vasodilation due to hypoxia
c) Increased central venous pressure (CVP) and impaired cerebral venous drainage
d) A systemic inflammatory response to carbon dioxide
-
According to the standardized technique, at what distance posterior to the globe should the ONSD be measured?
a) 1 mm
b) 3 mm
c) 5 mm
d) At the point of maximal diameter
-
The anatomical basis for using ONSD to estimate ICP relies on the direct communication between the intracranial subarachnoid space and which structure?
a) The vitreous humor
b) The subarachnoid space surrounding the optic nerve
c) The central retinal artery
d) The cavernous sinus
-
The 2026 clinical trial on patients undergoing laparoscopic prostatectomy investigated the effect of which prophylactic intervention on ONSD?
a) Hypertonic saline
b) Acetazolamide
c) Propofol infusion
d) Mannitol
-
What was the primary conclusion of the 2026 mannitol study discussed in the lecture?
a) Mannitol effectively prevented the ONSD increase during Trendelenburg positioning.
b) Mannitol significantly reduced ONSD, but only after 6 hours.
c) Mannitol did not significantly alter the ONSD increase caused by the Trendelenburg position.
d) The study was inconclusive due to poor image quality.
-
Which patient position is known to cause a significant and progressive increase in ONSD during prolonged surgery?
a) Reverse Trendelenburg
b) Lateral decubitus
c) Trendelenburg
d) Supine with head neutral
-
To ensure patient safety during ONSD ultrasonography, what should be placed between the transducer and the closed eyelid?
a) A small amount of saline
b) A sterile transparent dressing
c) A dry gauze pad
d) Nothing, direct contact is acceptable with sterile gel
-
Which pre-existing condition is highlighted as a critical consideration due to its effect on intraocular pressure?
a) Cataracts
b) Myopia
c) Closed-angle glaucoma
d) Macular degeneration
-
A patient is unresponsive one hour after an 8-hour surgery. An ONSD measurement is 6.3 mm. What is the most appropriate next step based on this finding?
a) Administer a reversal agent immediately.
b) Extubate the patient and move to the recovery room.
c) Keep the patient intubated and transfer to the ICU for observation.
d) Wait another hour before taking any action.
-
What type of ultrasound transducer is recommended for ONSD measurement?
a) Low-frequency curvilinear transducer
b) Phased array transducer
c) High-frequency linear transducer
d) Endocavitary transducer
-
What is a common postoperative symptom attributed to elevated intraoperative ICP?
a) Hypothermia
b) Bradycardia
c) Headache and agitation
d) Polyuria
-
A patient with which of the following conditions would be considered at highest risk for complications from ICP elevation during laparoscopic surgery?
a) Well-controlled hypertension
b) A history of prior neurosurgery
c) Mild asthma
d) Osteoarthritis
-
The lecture emphasizes that the most clinically significant aspect of ONSD measurement is:
a) The absolute value from a single measurement.
b) The difference in diameter between the left and right eye.
c) The evolution of the measurement over time (the trend).
d) The measurement obtained only in the dominant eye.
-
Why is ONSD measurement less reliable in infants under one year of age?
a) Their optic nerves are not fully myelinated.
b) Open fontanelles provide compliance, buffering increases in ICP.
c) The globe is too small for accurate probe placement.
d) Ultrasound waves cannot penetrate the infant skull.
-
What is the recommended action if ONSD measurements between the right and left eyes differ by more than 0.5 mm?
a) Average the two values and proceed.
b) Use the higher of the two values.
c) Repeat the measurements as it may indicate a technical error.
d) Document the discrepancy and use the right eye's value.
-
Which physiological effect of hypercapnia most directly contributes to elevated ICP?
a) Increased heart rate
b) Cerebral vasodilation
c) Decreased mean arterial pressure
d) Bronchoconstriction
-
In the sonographic image of the optic nerve, what does the bright, hyperechoic outer layer represent?
a) The optic nerve fibers
b) The arachnoid mater
c) The dura mater
d) The posterior sclera
-
According to the lecture, the learning curve to achieve proficiency in ONSD measurement is approximately:
a) 5-10 scans
b) 25-30 scans
c) 50-60 scans
d) Over 100 scans
-
All of the following contribute to increased ICP in the described surgical scenario EXCEPT:
a) Pneumoperitoneum
b) Hypercapnia
c) Trendelenburg position
d) Reverse Trendelenburg position
-
A postoperative ONSD reading provides what benefit in a medicolegal context for a patient with delayed emergence?
a) A definitive diagnosis of stroke
b) Proof of surgical error
c) A reason to re-operate immediately
d) Objective data supporting a clinical decision for a higher level of care
Correct Answers:
1.c, 2.b, 3.b, 4.d, 5.c, 6.c, 7.b, 8.c, 9.c, 10.c, 11.c, 12.b, 13.c, 14.b, 15.c, 16.b, 17.c, 18.b, 19.d, 20.d
MOTIVATIONAL MESSAGE FROM DR. R. K. MISHRA
The mark of a great surgeon is not merely the skill in their hands, but the relentless curiosity in their mind. Never cease to question, to learn, and to integrate new knowledge, for this is the discipline that turns good outcomes into excellent ones.
May you continue to pursue this path of constant improvement with dedication and wisdom. My best wishes are with you.
| Older Post | Home | Newer Post |





