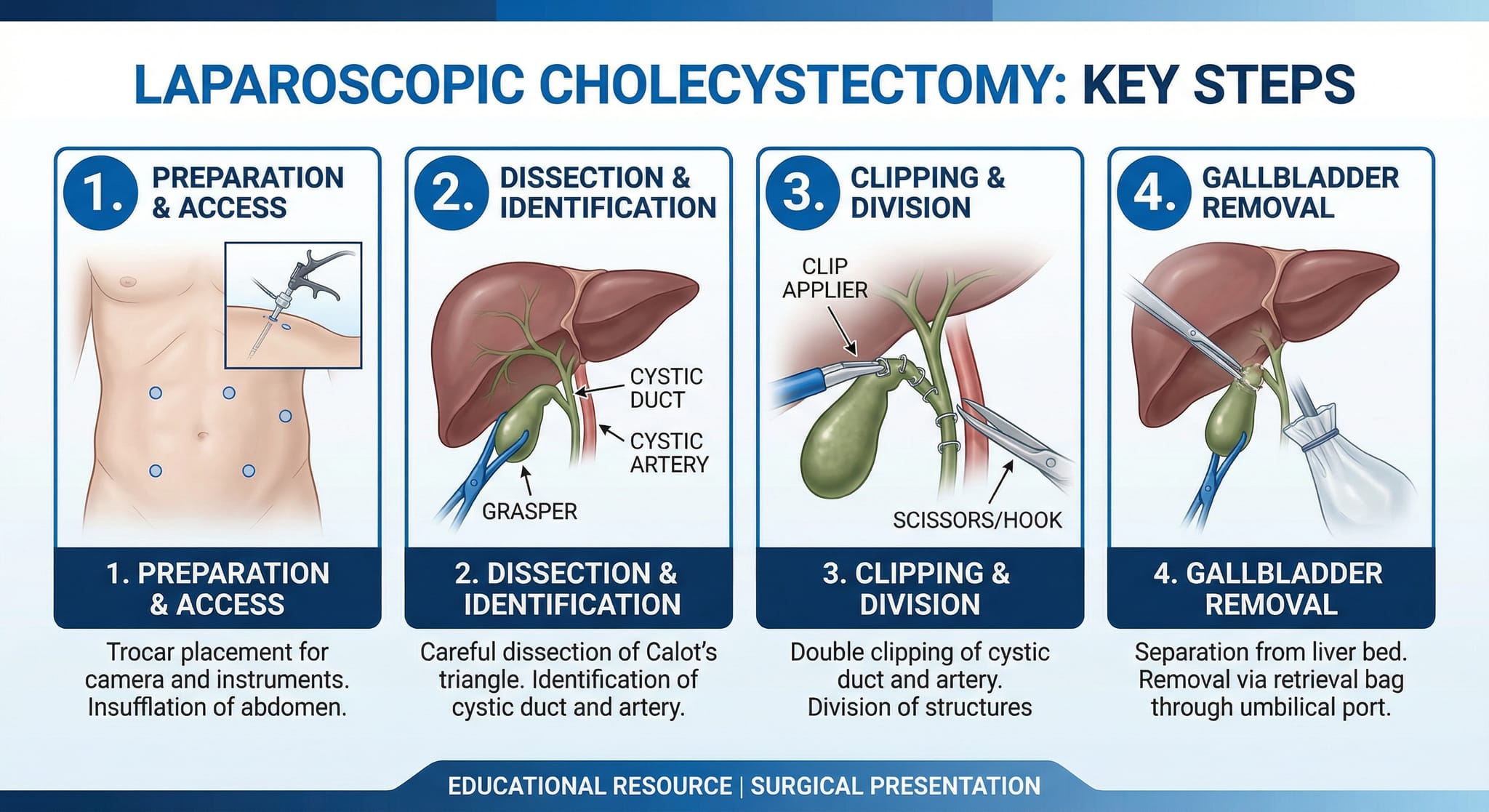
PRINCIPLES AND TECHNIQUES OF SAFE LAPAROSCOPIC CHOLECYSTECTOMY
BASIC INFORMATION
Date & Time: Friday, 6 February 2026 (Indian Standard Time)Lecture Handout Prepared from the Teaching Session by: Dr. R. K. Mishra
SUMMARY
This lecture provides a comprehensive overview of the principles and standardized techniques for performing a safe laparoscopic cholecystectomy. It establishes laparoscopic cholecystectomy as the gold standard for managing gallstone disease and details its historical context and pivotal role in popularizing minimally invasive surgery. The core of the lecture is a systematic approach designed to minimize complications, particularly common bile duct (CBD) injury. This includes preoperative assessment using the "First View of the Gallbladder" to predict surgical difficulty, a detailed review of surgical anatomy, and the disciplined application of the Critical View of Safety (CVS).
The session covers patient positioning, port placement for both American and French techniques, and the steps for establishing pneumoperitoneum. Key dissection principles are emphasized, such as the posterior-first approach and the importance of anatomical landmarks like Rouvier's sulcus. Advanced techniques, including extracorporeal knot tying, the use of Indocyanine Green (ICG) fluorescence cholangiography, and specimen retrieval methods, are discussed in detail. The lecture also addresses the management of complications, evidence-based practices regarding surgical drains, and specific considerations for pediatric patients, providing a complete framework for surgeons in training.
KEY KNOWLEDGE POINTS
- Laparoscopic cholecystectomy is the undisputed gold standard for treating gallstone disease.
- The "First View of the Gallbladder" (liver edge morphology, fundal projection, subcostal space) is a predictive tool for surgical difficulty.
- The Critical View of Safety (CVS) is the most critical step for preventing bile duct injury and requires the creation of anterior and posterior windows, skeletonization of the cystic pedicle, and dissection of the gallbladder from the liver bed.
- Anatomical landmarks, particularly Rouvier's sulcus, and specific traction techniques (e.g., anterolateral traction on Hartmann's pouch) are essential for safe dissection.
- Indocyanine Green (ICG) near-infrared fluorescence cholangiography is a modern, real-time, radiation-free adjunct for delineating biliary anatomy and enhancing safety.
- Extracorporeal knot tying is a valuable skill, offering a safe alternative to metallic clips, especially in cases with a short, wide, or inflamed cystic duct.
- Routine use of commercial endobags for gallbladder retrieval is the standard of care to prevent port-site infection and metastasis.
- The routine placement of surgical drains after uncomplicated cholecystectomy is not supported by evidence and should be avoided.
- Surgeons must understand the proper use and limitations of energy devices, such as the Harmonic Scalpel, especially in the context of device reuse.
Laparoscopic cholecystectomy is one of the most frequently performed procedures in general surgery, with approximately 40,000 performed globally each day. It is universally recognized as the "gold standard" for managing gallstone disease and was instrumental in transforming laparoscopy from a diagnostic tool into a mainstream therapeutic modality. While often straightforward, the procedure can present significant challenges, and iatrogenic bile duct injury remains a devastating complication. A thorough understanding of anatomy, adherence to standardized safety protocols, and a meticulous surgical technique are paramount. This lecture outlines a systematic approach to laparoscopic cholecystectomy, focusing on the foundational principles of safe dissection, the establishment of the Critical View of Safety, and the integration of modern technologies to ensure patient safety and optimal outcomes.
LEARNING OBJECTIVES
- To understand the historical significance and established role of laparoscopic cholecystectomy in modern surgery.
- To master the preoperative assessment of surgical difficulty using the "First View of the Gallbladder."
- To differentiate the anatomical boundaries of Calot's triangle in laparoscopic versus open surgery and utilize landmarks like Rouvier's sulcus.
- To learn the standardized technique for safe dissection and ligation of the cystic duct and artery to achieve the Critical View of Safety and prevent common bile duct injury.
- To compare and contrast the American and French positions for laparoscopic cholecystectomy, including ergonomic port placement strategies.
- To comprehend the principles and practical application of Indocyanine Green (ICG) fluorescence cholangiography.
- To evaluate the evidence-based best practices for gallbladder retrieval, use of surgical drains, and cystic duct ligation techniques.
1. Historical Context
The first laparoscopic cholecystectomy was performed by Dr. Erich Mühe of Germany in 1985. The procedure was instrumental in popularizing minimally invasive surgery worldwide, a movement significantly advanced in India by Dr. Pradeep Kumar Chaubey, who is widely regarded as the father of laparoscopy in the subcontinent.
2. Indications for Laparoscopic Cholecystectomy
While traditionally indicated for symptomatic disease, the modern paradigm is shifting due to the safety and minimal morbidity of laparoscopy.
- Primary Indication: Symptomatic cholelithiasis.
- Other Indications: Mucocele or empyema, cholesterosis, typhoid carriers, porcelain gallbladder, acute cholecystitis, and adenomatous gallbladder polyps.
- Asymptomatic Cholelithiasis: There is a growing consensus for prophylactic cholecystectomy in asymptomatic patients. Waiting for symptoms can increase the risk of complications (e.g., adhesions, frozen Calot's, Mirizzi syndrome) by up to five times, making subsequent surgery more difficult and hazardous.
3.1. The "First View of the Gallbladder"
Upon initial laparoscopic inspection, three observations help predict surgical difficulty:
- Inferior Surface of the Liver: A thin, wavy liver edge suggests an easy procedure, while a thick, straight edge indicates a fibrotic or fatty liver, leading to difficult exposure.
- Projection of the Gallbladder Fundus: A fundus projecting beyond the liver margin allows for easy retraction. If the fundus is intrahepatic, a dedicated liver retractor (e.g., Nathanson) is required.
- Subcostal Space: A distance of 6 cm or more between the rib cage and the liver provides ample room for manipulation. Less than 6 cm restricts movement and exposure.
Male patients often present a more challenging procedure due to a flatter chest anatomy, reduced subcostal space, and a larger, heavier, and more fibrotic liver.
4. Surgical Positioning, Pneumoperitoneum, and Port Placement
4.1. Surgical Positioning
- American Position: The surgeon stands on the patient's left side. This is the most common approach in Asia.
- French Position: The surgeon stands between the patient's legs. This position is considered more ergonomic, offering more favorable azimuth angles (contralateral setup).
Safe abdominal access is achieved using a Veress needle inserted in the inferior umbilical crease. Entry is confirmed with the irrigation, suction, and hanging drop tests. Insufflation should begin at a low flow rate (1 L/min), with the surgeon monitoring the quadromanometric indicator.
4.3. Port Placement (American Position)
- Primary/Optical Port (10 mm): In the inferior umbilical crease, preferably through the obliterated vitellointestinal tract to minimize hernia risk.
- Epigastric Port (10 mm): Just below the xiphoid process, piercing the membranous part of the falciform ligament. This is the main working port and accommodates the clip applicator.
- Right Mid-clavicular Port (5 mm): Below the costal margin, used for grasping Hartmann's pouch.
- Anterior Axillary Port (5 mm): Approximately 7.5 cm lateral and inferior to the third port, used for fundal retraction.
5. Principles of Safe Dissection and the Critical View of Safety (CVS)
5.1. Anatomical Landmarks and Dissection Principles
- Rouvier's Sulcus: A fissure on the liver surface, present in ~80% of patients. Dissection must remain superior to this landmark to avoid the porta hepatis and CBD.
- Posterior-First Dissection: A posterior-to-anterior dissection sequence is recommended. This approach exposes Rouvier's sulcus early and ensures that if bleeding occurs from an anterior vessel, blood flows away from the dissection field.
- Dissection Planes: Adhere to the principles of "white is right" (dissecting in avascular fascial planes) and "fat belongs to the organ" to minimize bleeding.
The CVS is the standard of care for preventing CBD injury. It requires three mandatory components:
- The hepatocystic triangle (Calot's triangle) is cleared of all fibrofatty tissue.
- The inferior one-third of the gallbladder is dissected from the liver bed (cystic plate).
- Two, and only two, structures are seen entering the gallbladder (the cystic duct and cystic artery).
6. Ligation Techniques: Clips, Knots, and Energy Devices
6.1. Safe Clipping and Ligation
- Cystic Duct: Clips must be applied on the spiral part of the duct, where the valves of Heister prevent slippage. A stump of 3-5 mm should be left from the CBD to avoid "lateral clipping" (inadvertent occlusion of the CBD). Apply two clips on the patient side and one on the specimen side.
- Cystic Artery: The artery should be clipped as close to the gallbladder wall as possible to minimize the risk of injuring the right hepatic artery.
- Extracorporeal Knot Tying: A slip knot (e.g., Meltzer's or Mishra's knot) is a safe alternative to clips, especially for a short, wide, or inflamed cystic duct. A key advantage is that it cannot cause lateral clipping.
The Harmonic Scalpel can seal vessels and ducts up to 5 mm. While effective for "clipless" cholecystectomy, it is contraindicated if the device is reused. The Teflon pad on the inactive jaw degrades with reuse, compromising coagulation and leading to a high risk of hemorrhage or bile leak.
7. Intraoperative Cholangiography: ICG Fluorescence
Conventional C-arm cholangiography is now considered obsolete due to radiation exposure and its cumbersome nature.
- Near-Infrared Fluorescence with ICG: This is the modern gold standard. A 2.5 mg dose of Indocyanine Green (ICG) is injected intravenously 45 minutes preoperatively. The dye is excreted in bile, and when viewed with an NIR-enabled camera, it provides a real-time, radiation-free, dynamic map of the entire biliary tree. It is a powerful safety adjunct for confirming anatomy before ligation.
- Cost-Saving Strategy: A 25 mg vial can be aseptically divided into 10 single-dose vials, significantly reducing the per-patient cost.
8.1. Gallbladder Retrieval
The use of a commercial, tear-resistant endobag is the standard of care. This prevents port-site contamination, infection, stone spillage, and port-site metastasis in cases of incidental gallbladder carcinoma. Improvised glove bags are unreliable, prone to puncture, and can cause a foreign body reaction if fragments are retained.
8.2. Surgical Drains
Routine placement of a surgical drain after uncomplicated cholecystectomy is not supported by evidence. Drains do not prevent complications, may create a false sense of security, and can cause harm by dislodging clips or introducing retrograde infection. A drain should only be placed selectively in cases of significant intraoperative concern and should be positioned in the subhepatic space (Morrison's pouch), away from the clips.
9. Pediatric Laparoscopic Cholecystectomy
The surgical principles are identical to adults, but require modification.
- Insufflation Pressure: Lower pressure is used (e.g., 8 mmHg).
- Instrumentation: Pediatric-length instruments are ideal.
- Technique: The smaller, more delicate structures demand greater precision. Clipless cholecystectomy with a Harmonic Scalpel is often feasible as the cystic duct is typically <5 mm.
- A thin, wavy liver edge and a projecting gallbladder fundus predict an easier cholecystectomy. Be prepared for a difficult case in male patients.
- To avoid lateral clipping, always apply clips on the spiral part of the cystic duct, leaving a 3-5 mm stump. For a short or wide duct, an extracorporeal knot is a safer alternative.
- Anterolateral traction on Hartmann's pouch, not fundal pull, is the key to opening Calot's triangle and preventing CBD tenting.
- Always perform a final, meticulous inspection for bleeding or bile leakage before the gallbladder is fully detached from the liver bed.
- Practice advanced skills like knot tying in routine cases to ensure proficiency for complex situations.
- Do not perform a clipless cholecystectomy with a reused Harmonic Scalpel; the risk of failed sealing is unacceptably high.
- Embrace ICG fluorescence cholangiography as a routine safety measure to provide an anatomical "road map" and increase surgical confidence.
- Avoid the routine use of surgical drains. Trust the evidence and your dissection.
- Intraoperative:
- Common Bile Duct (CBD) Injury: The most serious complication, often caused by misidentification of anatomy. Prevention relies on achieving the CVS, augmented by ICG.
- Right Hepatic Artery Injury: Risk is minimized by clipping the cystic artery close to the gallbladder. If injury is suspected, the liver must be monitored for ischemia; a hepatobiliary consult for potential revascularization is required if the liver turns cyanotic.
- Gallbladder Perforation: Requires meticulous suction of spilled bile and retrieval of lost stones to prevent abscess formation.
- Early Postoperative:
- Bile Leak: From the cystic duct stump or an accessory duct (of Luschka).
- Hemorrhage: From the cystic artery stump or liver bed.
- Subhepatic Abscess: Often a consequence of a bile leak or retained stones.
- Late Postoperative:
- Biliary Stricture: Can result from ischemic or thermal injury to the CBD.
- Cystic Duct Stump Stone ("Cat-eye Stone"): Forms when a clip on a dilated cystic duct stump acts as a nidus for stone formation.
- Achieving and documenting the Critical View of Safety is the standard of care and the best defense against medicolegal challenges.
- Failure to use an endobag for specimen retrieval, leading to port-site infection or metastasis, can have significant medicolegal implications.
- The use of ICG fluorescence is rapidly becoming the standard of care in complex cases, and its omission may be questioned if a bile duct injury occurs.
- Prophylactic cholecystectomy for asymptomatic gallstones is a valid clinical argument, as waiting for symptoms increases complication rates.
- Preoperative MRCP is indicated for patients with abnormal liver function tests or concerning ultrasound findings (e.g., dilated CBD > 9 mm, thickened gallbladder wall > 3 mm).
- Laparoscopic cholecystectomy is the gold standard, but its safety depends on rigorous preoperative assessment and adherence to a standardized surgical technique.
- The Critical View of Safety is non-negotiable. It is achieved through meticulous dissection, proper traction, and creation of clear anterior and posterior windows.
- Modern adjuncts like ICG fluorescence cholangiography provide a real-time anatomical road map, significantly enhancing safety and reducing the risk of bile duct injury.
- Mastery of advanced skills, including extracorporeal knot tying, and adherence to evidence-based practices regarding drains and specimen retrieval are hallmarks of a proficient laparoscopic surgeon.
- Never ligate or divide a structure without being absolutely certain of its identity. The goal is to prove what the structure is not (i.e., not the CBD) before proceeding.
1. According to the "First View of the Gallbladder," which finding suggests a more difficult surgery?
a) A thin and wavy liver edge
b) A thick and straight liver edge
c) The gallbladder fundus projecting beyond the liver margin
d) A subcostal space of 7 cm
2. Which traction technique is most effective for opening Calot's triangle and preventing CBD tenting?
a) Fundal pull towards the right shoulder
b) Posterior pressure on the gallbladder body
c) Anterolateral traction on Hartmann's pouch
d) Medial traction on the fundus
3. What is the superior boundary of the Calot's triangle in laparoscopic surgery?
a) Cystic artery
b) Common hepatic duct
c) Inferior surface of the liver (cystic plate)
d) Right hepatic artery
4. To avoid "lateral clipping," what is the recommended minimum distance to maintain from the CBD when applying a clip to the cystic duct?
a) Flush with the CBD
b) 1 mm
c) 3-5 mm
d) 10 mm
5. Which of the following is a mandatory component of the Critical View of Safety?
a) Visualizing the common bile duct throughout the dissection
b) Identifying and preserving the lymph node of Lund
c) Dissecting the inferior one-third of the gallbladder off the liver bed
d) Performing an intraoperative cholangiogram
6. In which scenario is an extracorporeal slip knot considered a safer alternative to a metallic clip?
a) For ligating the cystic artery
b) When the cystic duct is very long and thin
c) When the cystic duct is short and wide
d) In all pediatric cases
7. What is a primary advantage of ICG fluorescence cholangiography over conventional C-arm cholangiography?
a) It provides a single high-resolution image.
b) It does not require a special camera system.
c) It provides real-time, dynamic visualization without radiation.
d) It is less expensive to perform.
8. For routine ICG cholangiography to visualize bile ducts, when should the ICG be injected?
a) Intraoperatively, 2 minutes before visualization
b) 45 minutes preoperatively via a peripheral vein
c) Locally into the gallbladder wall
d) 24 hours before surgery
9. What is the current evidence-based recommendation for using surgical drains after routine laparoscopic cholecystectomy?
a) A drain should always be placed in Calot's triangle.
b) Routine use should be avoided as it offers no benefit and may cause harm.
c) A drain is required if the surgery lasts longer than one hour.
d) Two drains should be placed in Morrison's pouch.
10. The use of a Harmonic Scalpel for "clipless" cholecystectomy is contraindicated in which situation?
a) In all pediatric patients
b) When the cystic artery is larger than 3 mm
c) When the device has been reused and its Teflon pad is degraded
d) In cases of acute cholecystitis
11. Dissection must be kept superior to which anatomical landmark to avoid injury to the porta hepatis?
a) Foramen of Winslow
b) Falciform ligament
c) Morrison's pouch
d) Rouvier's sulcus
12. In the American position for laparoscopic cholecystectomy, where does the primary surgeon stand?
a) On the patient's right side
b) Between the patient's legs
c) On the patient's left side
d) At the head of the patient
13. What is the primary reason for using a commercial endobag for gallbladder retrieval?
a) It is reusable for multiple patients.
b) It is made of a biodegradable material.
c) It prevents port-site contamination, infection, and metastasis.
d) It is the most cost-effective option.
14. A late complication known as a "cat-eye stone" is associated with:
a) Spilled gallstones in the peritoneum
b) A retained stone in the common bile duct
c) Improper clip application on a dilated cystic duct stump
d) Thermal injury to the gallbladder bed
15. To minimize the risk of injuring the right hepatic artery, the cystic artery should be ligated:
a) As close to its origin as possible
b) As close to the gallbladder wall as possible
c) In its middle portion, after dividing the cystic duct
d) Using an extracorporeal knot instead of clips
16. The "nipple effect" refers to the appearance of which structures after releasing traction on Hartmann's pouch?
a) The tented common bile duct
b) The right and left hepatic ducts
c) The erect, true cystic duct and artery
d) The fundus of the gallbladder
17. When placing the epigastric port, which part of the falciform ligament should be pierced to avoid complications?
a) The fatty, inferior part
b) The ligamentum teres
c) The avascular, membranous (upper) part
d) The coronary ligament
18. A posterior-first dissection approach is considered safer primarily because:
a) It allows for early ligation of the cystic artery.
b) Variant arteries are most common posteriorly.
c) It exposes Rouvier's sulcus early and directs potential bleeding away from the field.
d) It is a faster technique than an anterior-first approach.
19. Who is credited by the global surgical community for performing the first laparoscopic cholecystectomy?
a) Philippe Mouret
b) Erich Mühe
c) Pradeep Kumar Chaubey
d) Dr. R. K. Mishra
20. What is a key difference in performing laparoscopic cholecystectomy in a pediatric patient compared to an adult?
a) The surgical steps are entirely different.
b) A lower pneumoperitoneum pressure (e.g., 8 mmHg) is used.
c) The Critical View of Safety is not required.
d) The gallbladder is always removed without an endobag.
The mastery of surgery is a covenant between your hands and your mind. Train your hands through relentless practice, but enlighten your mind with ceaseless learning, for it is the prepared mind that guides the scalpel toward healing and away from harm.
May you operate with the wisdom of your preparation and the humility to always learn more. I wish you all clarity and success in your surgical careers.
No comments posted...
| Older Post | Home | Newer Post |





