Prof. Dr. R. K. Mishra
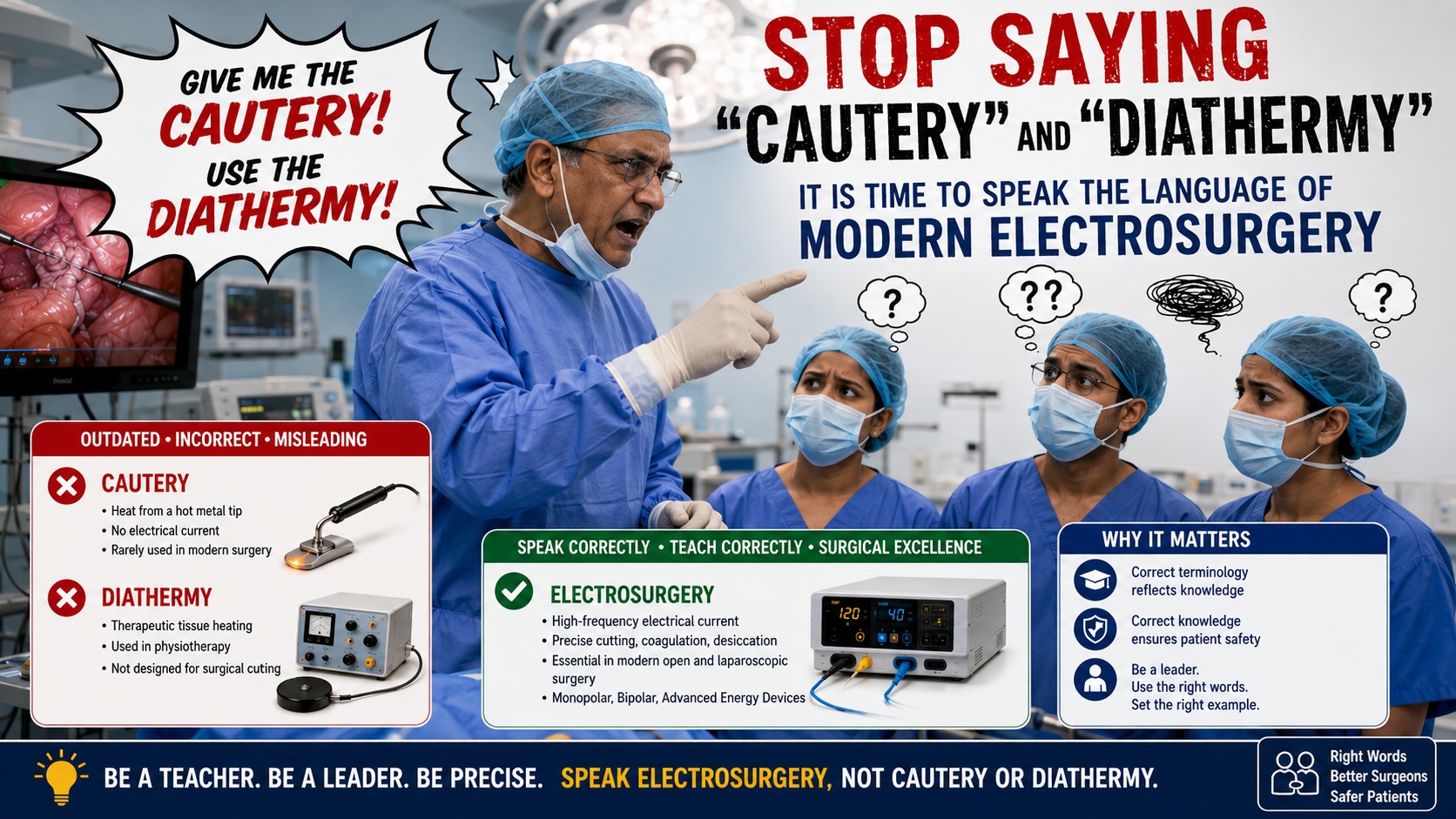
Language shapes knowledge. In surgery, precise terminology reflects precise understanding. Yet in operating rooms across the world, one continues to hear phrases such as “Give me the diathermy,” “Pass the cautery,” or “Use cautery here.” These expressions have become so deeply embedded in surgical culture that even experienced surgeons, professors, and trainers frequently use them without recognizing their scientific inaccuracy.
This practice is particularly concerning because modern surgeons are not using cautery devices, nor are they primarily performing diathermy. They are using sophisticated electrosurgical units (ESUs) that operate on principles fundamentally different from both traditional cautery and classical medical diathermy. As educators and leaders in surgery, we have a responsibility to teach the correct terminology and the correct science to the next generation.
The Problem with Surgical Language
Imagine a pilot referring to a modern glass-cockpit aircraft as a “flying machine,” or a cardiologist calling a transcatheter valve replacement “heart plumbing.” Such terminology would immediately appear outdated and imprecise.
Yet in surgery, highly trained professionals continue to refer to advanced electrosurgical instruments as “cautery” and electrosurgical generators as “diathermy machines.” The problem is not merely semantic. Incorrect terminology reflects incomplete understanding of the technology being used and can hinder effective teaching of surgical energy safety.
When a surgeon says, “Give me the cautery,” what is actually being requested?
Is it a monopolar hook electrode?
A spatula electrode?
A needle electrode?
A bipolar forceps?
An advanced vessel-sealing device?
All of these are different instruments utilizing different energy delivery systems. Calling them collectively “cautery” is scientifically inaccurate.
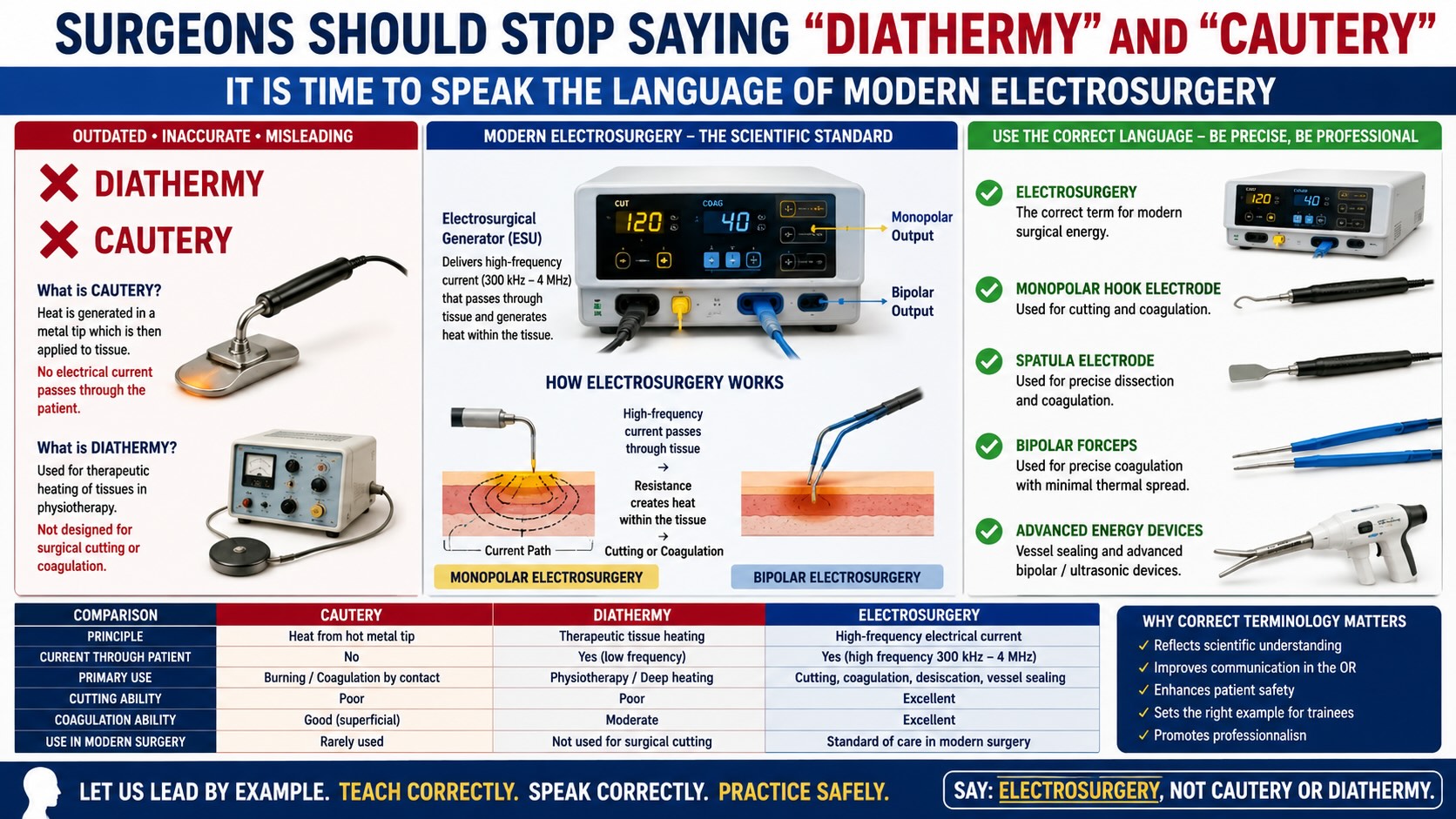
What Is True Cautery?
Cautery is one of the oldest surgical technologies known to medicine. No more availanle.
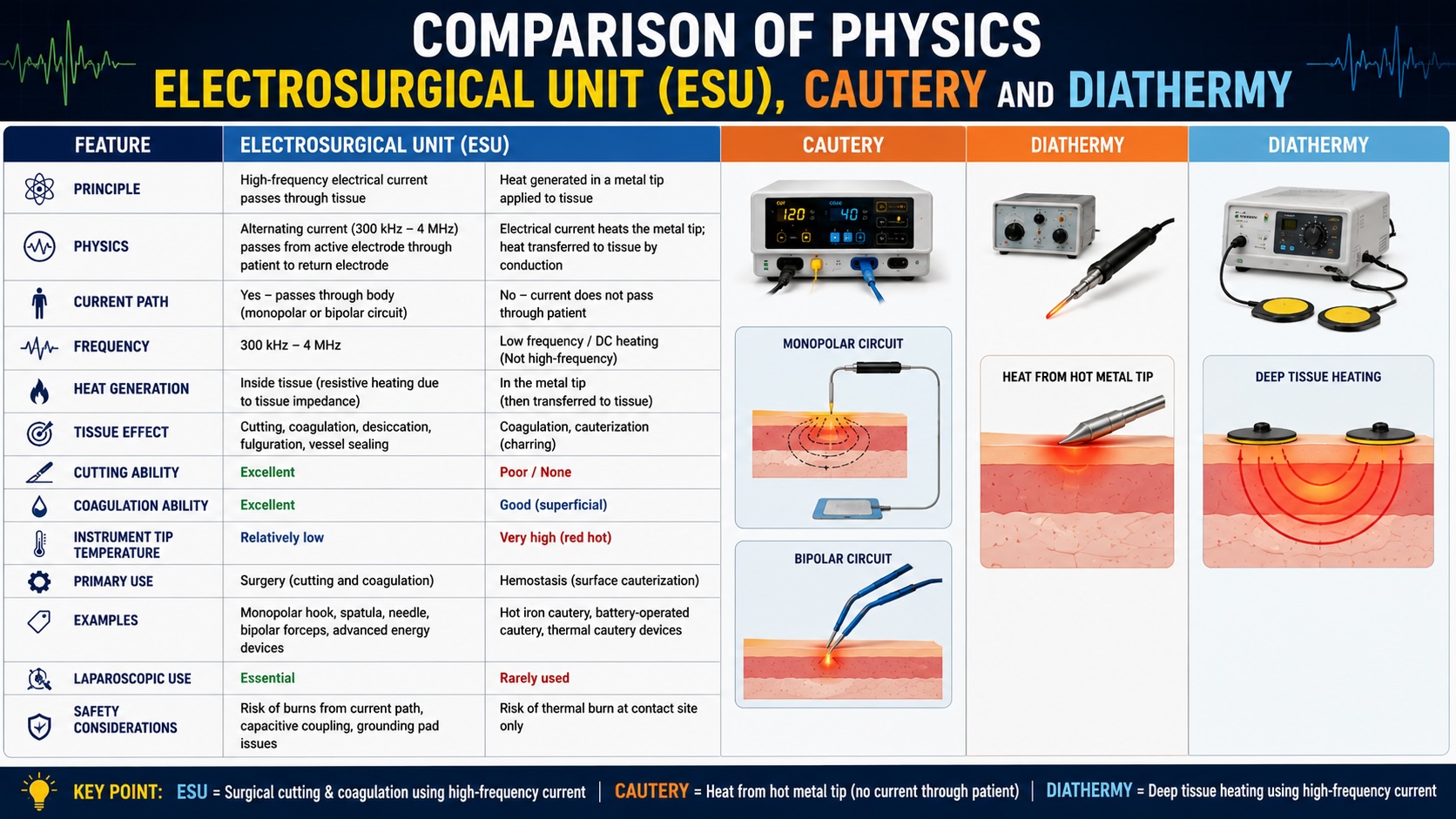
In true cautery, a metal instrument is heated externally and then applied to tissue. The heated metal burns or coagulates tissue by direct thermal transfer.
Examples include:
-
Hot iron cautery used in ancient surgery
-
Battery-powered ophthalmic cautery
-
Thermal cautery devices in ENT surgery
-
Disposable handheld cautery pens
The defining characteristic of cautery is simple:
No electrical current passes through the patient.
The instrument becomes hot, and that heat is transferred to tissue.
This is fundamentally different from modern electrosurgery.
What Is Diathermy?
The word diathermy originates from the Greek words:
-
Dia = through
-
Therme = heat
Diathermy literally means “heating through tissue.” No more manufacture by reputed company.
Some professors can perform a flawless laparoscopic hysterectomy, navigate the ureter in dense endometriosis, and quote surgical literature from memory—yet the moment they reach for an energy device, they proudly announce, “Give me the cautery!” A puzzled biomedical engineer faints quietly in the corner while the electrosurgical generator, capable of delivering precisely controlled high-frequency current, wonders why it is still being called by the name of a nineteenth-century hot iron. The residents dare not object; after all, the same professor who lectures on evidence-based medicine still insists on calling a monopolar hook “diathermy.” Thus, generation after generation of trainees inherit the sacred tradition of using state-of-the-art electrosurgery while speaking the language of medieval blacksmiths. If surgical terminology had a museum, “cautery” and “diathermy” would be valuable historical exhibits—not daily operating room commands.
Historically, physicians discovered that high-frequency alternating current could generate heat within tissues without producing painful muscle contractions. This phenomenon became known as diathermy.
Classical diathermy was primarily used for:
-
Deep tissue heating
-
Physiotherapy
-
Rehabilitation medicine
-
Musculoskeletal pain treatment
The purpose was therapeutic heating rather than tissue cutting.
Although electrosurgery also produces tissue heating, modern electrosurgical systems were developed specifically to create controlled surgical effects such as cutting, coagulation, desiccation, and fulguration.
Therefore, electrosurgery evolved beyond traditional diathermy.
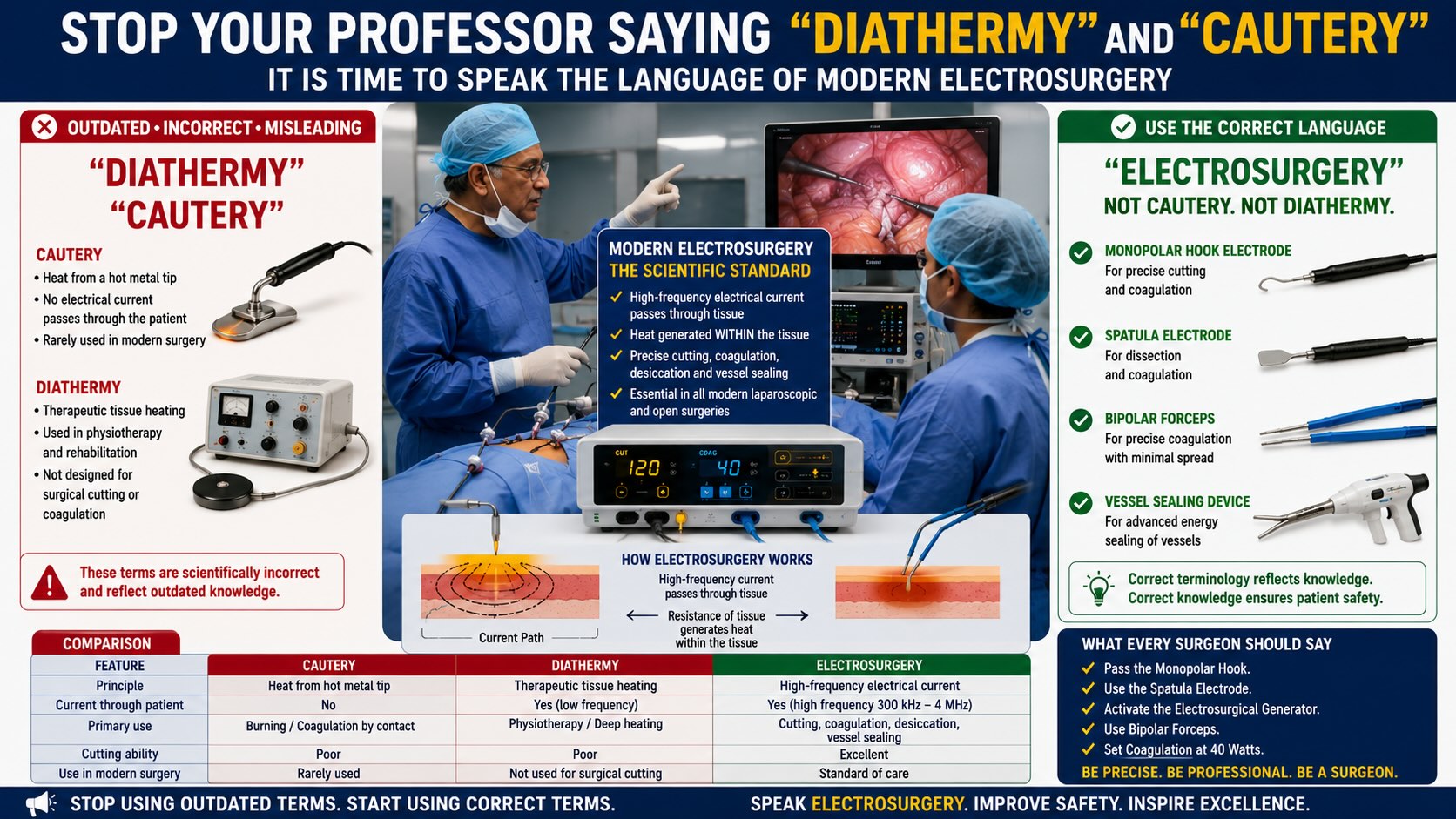
What Is Electrosurgery?
Electrosurgery uses high-frequency alternating current, typically between 300 kHz and 3.3 MHz, to create desired tissue effects.
The electrosurgical generator produces electrical energy that passes through tissue.
As tissue resists the flow of current, intracellular water rapidly heats and vaporizes, producing different effects depending on current density and waveform.
These effects include:
-
Cutting
-
Coagulation
-
Desiccation
-
Fulguration
-
Vessel sealing
Unlike cautery, the electrode itself usually remains relatively cool.
The heat is generated within the tissue, not within the instrument.
This distinction is crucial.
Physics Comparison

From a scientific standpoint, the laparoscopic hook used during cholecystectomy is not a cautery instrument. It is a monopolar electrosurgical electrode.
Unfortunately, many senior surgeons and professors who trained decades ago have not kept pace with the rapid evolution of surgical energy technology. While they remain highly skilled clinicians and operators, some continue to use outdated terms such as “cautery” and “diathermy” when referring to modern electrosurgical systems. This is not merely a linguistic issue; it reflects a gap between contemporary surgical science and traditional teaching. Today's electrosurgical generators incorporate sophisticated waveform modulation, tissue sensing, vessel-sealing algorithms, and advanced safety mechanisms that differ fundamentally from classical cautery and diathermy. As educators, professors have a responsibility to continuously update their knowledge, embrace current technology, and teach accurate terminology to trainees. Surgical excellence requires lifelong learning, and mastery of modern energy devices should be considered as important as mastery of surgical anatomy and technique.
Similarly, the spatula used during laparoscopic hysterectomy is not “diathermy.” It is an electrosurgical spatula electrode connected to an electrosurgical generator.
Why Correct Terminology Matters ?
Modern surgery increasingly emphasizes energy safety.
Complications such as:
-
Insulation failure
-
Capacitive coupling
-
Direct coupling
-
Alternate site burns
-
Thermal spread
-
Delayed bowel injury
are electrosurgical phenomena.
These complications cannot be properly understood if surgeons continue to think in terms of “cautery” instead of electrosurgery.
When residents hear “Use the cautery,” they learn a vague concept.
When they hear “Use the monopolar hook electrode in coagulation mode at 30 watts,” they learn surgical science.
Language influences education.
Education influences patient safety.
The Responsibility of Surgical Teachers
Perhaps the greatest disappointment is that incorrect terminology persists even among senior surgeons and educators.
Many consultants still instruct assistants:
“Give me the diathermy.”
“Use the cautery.”
“Keep the cautery ready.”
Rarely do we hear:
“Pass the monopolar hook electrode.”
“Activate the electrosurgical generator.”
“Use the bipolar forceps.”
“Switch to the spatula electrode.”
Young surgeons learn the language used by their mentors. If mentors continue using inaccurate terminology, generations of surgeons will continue repeating the same mistake.
Teaching correct terminology costs nothing but contributes enormously to scientific clarity.
A Call to Gynecologists and Laparoscopic Surgeons
Gynecologists have been among the pioneers of minimally invasive surgery. Total laparoscopic hysterectomy, endometriosis surgery, myomectomy, and oncologic procedures all rely heavily on advanced electrosurgical technology.
Therefore, gynecologists should be leaders in adopting correct terminology.
Instead of saying:
“Give me the cautery.”
say:
“Give me the monopolar hook.”
Instead of saying:
“Use the diathermy.”
say:
“Use electrosurgery.”
Instead of saying:
“Cauterize that vessel.”
say:
“Coagulate that vessel using bipolar electrosurgery.”
These changes may appear small, but they reflect a deeper understanding of modern surgical energy.
Conclusion
The operating room of the twenty-first century is driven by sophisticated electrosurgical technology. Continuing to describe these systems as “cautery” or “diathermy” is scientifically inaccurate and educationally counterproductive. Modern surgeons should embrace precise terminology that reflects the actual physics and function of the instruments they use.
The future surgeon should speak of electrosurgery, electrosurgical generators, monopolar electrodes, bipolar forceps, vessel-sealing systems, hook electrodes, and spatula electrodes—not cautery and not diathermy.
Precision in language promotes precision in thought. Precision in thought promotes precision in surgery. And precision in surgery ultimately improves patient safety.
It is time for the surgical community to retire outdated terminology and adopt the language of modern electrosurgery.
| Older Post | Home | Newer Post |





