BASIC INFORMATION:
Date & Time: 2026-06-09 18:53:39 IST
Lecture Handout Prepared from the Teaching Session by: Dr. R. K. Mishra
SUMMARY:
This lecture addresses gallbladder cancer (GBC) as a geographically heterogeneous but globally lethal malignancy, drawing on the text Gallbladder Cancer—Current Treatment Options (Shukla, Pandey, Dixit, eds.). The discussion emphasizes the stark contrast in incidence between low-prevalence regions (e.g., the United States, Western Europe) and high-prevalence regions (e.g., the Indo-Gangetic belt in India, Chile, Japan), with overall 5-year survival below 5%. Key risk determinants include large gallstones (>3 cm), chronic bacterial colonization (notably Salmonella typhi and Helicobacter species), and anomalous pancreaticobiliary junction (APBJ) causing pancreaticobiliary reflux. A noteworthy female predominance is explored, including the prognostic association of estrogen and progesterone receptor positivity with earlier-stage, more differentiated disease.
Clinically, GBC presents with non-specific biliary symptoms, often mimicking benign gallstone disease, which contributes to late diagnosis and frequent incidental detection after elective cholecystectomy. The T stage—particularly the distinction between T1a (lamina propria) and T1b (muscular invasion)—is the pivotal determinant of surgical strategy and prognosis, anchored in the gallbladder’s unique absence of a submucosa that facilitates early lymphovascular dissemination to liver segments IVb and V. Imaging escalates from ultrasound to contrast-enhanced CT, with MRI/MRCP in selected cases.
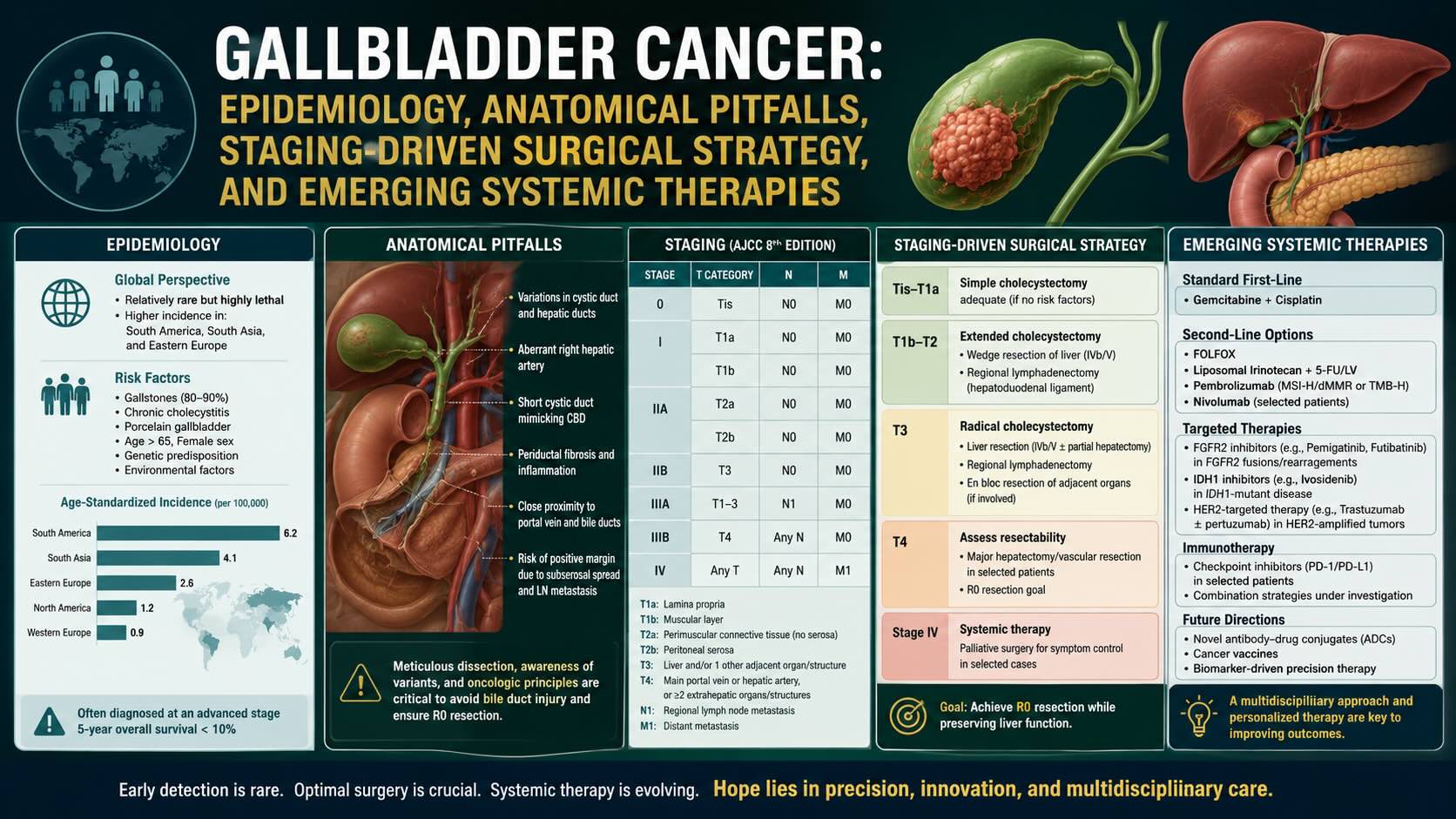
Curative intent relies on achieving R0 resection. Simple cholecystectomy suffices for T1a, whereas T1b and T2 require radical cholecystectomy (wedge resection of liver segments IVb and V with regional lymphadenectomy). Surgery is contraindicated in diffuse peritoneal spread or bilobar hepatic involvement. Adjuvant systemic therapy is important due to high recurrence (up to 70%); gemcitabine–cisplatin (ABCO2) sets the standard in advanced disease, and adjuvant capecitabine (BILCAP) improves survival after resection. Chemoradiation (e.g., SWOG S0809) may benefit R1 resections. Molecular therapeutics are emerging: HER2 amplification appears particularly relevant in GBC, with potential benefit from anti-HER2 strategies; EGFR-directed therapy has shown mixed results; anti-VEGF therapy may augment chemotherapy responses. Novel immunologic approaches targeting ELF3 frameshift neoantigens and epigenetic therapies aimed at reversing promoter hypermethylation of tumor suppressors (e.g., p16, PTEN) represent future directions. Routine histopathology of all gallbladder specimens is stressed to detect incidental, potentially curable disease.
KEY KNOWLEDGE POINTS:
-
GBC exhibits pronounced geographic variation; survival remains poor overall.
-
Major risk factors include large gallstones (>3 cm), chronic Salmonella typhi carriage, Helicobacter spp., and APBJ.
-
Female predominance is characteristic; ER/PR positivity correlates with earlier stage and better prognosis.
-
The gallbladder lacks a submucosa; invasion into muscle (T1b) markedly increases lymphovascular spread risk to liver segments IVb and V.
-
T staging dictates surgery: T1a—simple cholecystectomy; T1b/T2—radical cholecystectomy with liver wedge (IVb/V) and regional lymphadenectomy.
-
CT is the staging cornerstone; MRI/MRCP for ductal mapping; ultrasound is limited for early neoplasia.
-
Surgery is contraindicated with peritoneal carcinomatosis or bilobar liver involvement.
-
High recurrence necessitates systemic therapy: gemcitabine–cisplatin in advanced disease; adjuvant capecitabine after resection; chemoradiation may aid R1 margins.
-
Molecular targets: HER2 amplification (actionable), EGFR (variable), VEGF (anti-angiogenic adjuncts); emerging ELF3 neoantigen vaccines and epigenetic reprogramming.
-
Routine histopathology of all cholecystectomy specimens is essential to identify incidental GBC.
INTRODUCTION:
Gallbladder cancer is an aggressive malignancy with marked regional disparities in incidence and outcomes. Its lethality stems from silent early progression, non-specific symptoms, and unique anatomical features that facilitate early dissemination. Understanding risk determinants, anatomical vulnerabilities, and stage-based surgical decision-making is fundamental. Evolving systemic and molecular therapies aim to improve historically poor survival, while meticulous pathology practices enhance early detection of incidental, potentially curable disease.
LEARNING OBJECTIVES:
-
Describe epidemiological patterns and key risk factors for gallbladder cancer, including the roles of gallstone size, chronic infection, and APBJ.
-
Explain the anatomical and pathophysiological basis for T1a versus T1b staging implications and their surgical consequences.
-
Outline evidence-based management pathways, including indications for radical cholecystectomy, contraindications to surgery, and current systemic/adjuvant therapy strategies, with emerging molecular targets.
CORE CONTENT:
-
Epidemiology and Risk Determinants
1.1 Geographic Variation
-
Low incidence in the US and Western Europe; high incidence and mortality in the Indo-Gangetic belt, Chile, and Japan.
-
Overall 5-year survival remains <5%.
1.2 Gallstones and Carcinogenic Risk
-
Approximately 85% of GBC patients have gallstones; however, most patients with gallstones do not develop cancer.
-
Stone size is pivotal: stones >3 cm confer approximately a tenfold increased risk compared with smaller stones.
-
Mechanism: chronic mechanical mucosal trauma leading to persistent inflammation and carcinogenesis.
1.3 Chronic Infection
-
Salmonella typhi chronic carriage with biofilm formation on stones promotes sustained inflammation and DNA damage.
-
Helicobacter species implicated in chronic biliary irritation.
1.4 Anomalous Pancreaticobiliary Junction (APBJ)
-
Early union of bile and pancreatic ducts outside the duodenal wall permits pancreatic enzyme reflux into the biliary tree, chemically injuring gallbladder mucosa over years.
1.5 Sex Predilection and Hormonal Factors
-
Female predominance is unique among gastrointestinal malignancies.
-
Estrogen/progesterone receptor positivity correlates with earlier-stage disease and better prognosis, reflecting greater differentiation.
-
-
Clinical Presentation and Diagnostic Workup
2.1 Symptoms and Presentation
-
Non-specific symptoms: right upper quadrant pain, dyspepsia, fatty food intolerance—indistinguishable from benign biliary colic in early disease.
-
Advanced disease features: jaundice, weight loss, palpable mass—often unresectable at presentation.
-
High rate of incidental detection after elective cholecystectomy.
2.2 Imaging Strategy
-
Ultrasound: first-line for gallstones but limited in detecting early, flat neoplastic lesions; wall thickening is non-specific.
-
Contrast-enhanced CT: cornerstone for staging; evaluates hepatic invasion, vascular involvement, and nodal disease.
-
MRI/MRCP: utilized for delineating biliary anatomy and ductal involvement when indicated.
-
-
Pathological Staging and Anatomical Rationale
3.1 Critical Distinction: T1a vs T1b vs T2
-
T1a: invasion confined to lamina propria.
-
T1b: invasion into muscular layer.
-
T2: invasion through muscle into perimuscular connective tissue.
3.2 Anatomical Vulnerability
-
Absence of a submucosa in the gallbladder removes a defensive barrier to lymphovascular channels within the muscle.
-
Early access to lymphatics and veins predisposes to microscopic spread, particularly to liver segments IVb and V.
-
-
Operative Principles and Surgical Strategy
4.1 Goal of Surgery
-
Achieve R0 resection; positive margins (R1) portend high recurrence.
4.2 Incidental GBC Management
-
T1a (lamina propria only): simple cholecystectomy is adequate; long-term survival approaches 100%.
-
T1b (muscle invasion): mandates radical cholecystectomy—wedge resection of liver segments IVb and V with regional lymphadenectomy (porta hepatis/hepatoduodenal ligament nodes).
-
T2: managed as T1b with radical cholecystectomy and nodal dissection.
4.3 Contraindications to Curative Resection
-
Peritoneal carcinomatosis.
-
Bilobar hepatic involvement (diffuse disease across both lobes).
-
-
Systemic and Adjuvant Therapies
5.1 Recurrence Risk
-
Recurrence rates up to 70% after resection necessitate adjuvant strategies.
5.2 Chemotherapy Standards
-
Advanced/unresectable disease: gemcitabine plus cisplatin (ABCO2) improves survival versus gemcitabine alone (11.7 vs 8.1 months).
-
Adjuvant setting post-resection: capecitabine (BILCAP) associated with improved overall survival.
5.3 Chemoradiation in Margin-Positive Disease
-
Phase II data (SWOG S0809) suggest benefit of adjuvant chemoradiation, particularly in R1 resections, to sterilize the liver bed and margins.
-
-
Molecular and Emerging Therapeutic Targets
6.1 HER2 (ERBB2) Amplification
-
More prevalent in GBC than in other biliary tract cancers; anti-HER2 strategies (e.g., trastuzumab) combined with chemotherapy demonstrate enhanced cytotoxicity in amplified tumors.
6.2 EGFR Pathway
-
Overexpression reported with variability; trials of EGFR inhibitors (erlotinib, cetuximab) show mixed, modest benefits.
6.3 Angiogenesis (VEGF)
-
High VEGF-A expression supports anti-angiogenic therapy (e.g., bevacizumab) in combination with chemotherapy to improve response rates.
6.4 Neoantigen Vaccines (ELF3 Frameshift)
-
Regional variation in ELF3 frameshift mutations; these create neoantigens capable of eliciting CD8+ T-cell responses.
-
Peptide vaccine strategies represent precision immunotherapy in development.
6.5 Epigenetic Modulation
-
Hypermethylation-mediated silencing of tumor suppressors (e.g., p16, PTEN).
-
Epitherapy aims to reverse methylation and restore tumor suppressor function.
-
-
Pathology Practice and Systems Considerations
-
Routine histopathological examination of all cholecystectomy specimens is essential to detect incidental GBC.
-
Avoid cost-saving omissions that risk missing early, potentially curable disease.
-
SURGICAL PEARLS:
-
Always review the T category on incidental GBC pathology; T1b is a clear indication for re-resection with liver wedge (IVb/V) and lymphadenectomy.
-
The absence of submucosa explains early dissemination; do not underestimate T1b disease based on gross appearance.
-
Intraoperative discovery of peritoneal carcinomatosis or bilobar hepatic disease should prompt abandonment of curative resection and early transition to systemic therapy.
-
Achieve R0 margins; consider adjuvant chemoradiation for R1 resections.
-
Send every gallbladder specimen for histopathology, irrespective of intraoperative appearance.
ANESTHETIC AND PHYSIOLOGICAL CONSIDERATIONS:
-
Not specifically discussed in the lecture.
COMPLICATIONS AND THEIR MANAGEMENT:
-
Intraoperative: Not specifically itemized; principle is to avoid non-curative extensive resections in disseminated disease.
-
Early postoperative: Not detailed; emphasis placed on margin status and early initiation of adjuvant therapy where indicated.
-
Late postoperative: High recurrence risk up to 70%; managed with systemic therapy according to established protocols.
MEDICOLEGAL AND PATIENT SELECTION CONSIDERATIONS:
-
Ensure routine histopathology of all cholecystectomy specimens; failure to detect incidental GBC may delay definitive care.
-
Document thorough staging and clear rationale for operative decisions, especially when electing re-resection for T1b/T2 disease.
-
Recognize and document contraindications to surgery (peritoneal carcinomatosis, bilobar hepatic involvement) to avoid non-beneficial procedures.
SUMMARY AND TAKE-HOME MESSAGES:
-
Gallbladder cancer is geographically concentrated yet globally lethal; vigilance is required in high-risk populations.
-
The T1a versus T1b distinction is critical; T1b/T2 disease mandates radical cholecystectomy with hepatic wedge and nodal clearance.
-
Routine histopathology of all gallbladder specimens enables detection of incidental, potentially curable disease.
-
Systemic therapy has evolved: gemcitabine–cisplatin for advanced disease; adjuvant capecitabine post-resection; chemoradiation may benefit R1 cases.
-
Molecular advances, particularly HER2 targeting and ELF3 neoantigen vaccines, offer emerging therapeutic opportunities.
MULTIPLE CHOICE QUESTIONS (MCQs):
-
In regions such as the Indo-Gangetic belt, gallbladder cancer is best characterized as:
A. Rare and indolent
B. Highly prevalent and lethal
C. Decreasing in incidence
D. Primarily pediatric
Correct answer: B
-
The overall 5-year survival for gallbladder cancer is approximately:
A. 25%
B. 15%
C. <5%
D. 40%
Correct answer: C
-
Which risk factor confers an approximately tenfold increased risk of GBC?
A. Multiple small stones <5 mm
B. Porcelain gallbladder
C. Single cholesterol polyp
D. Gallstones >3 cm
Correct answer: D
-
Chronic Salmonella typhi carriage contributes to GBC risk primarily by:
A. Direct hepatocyte infection
B. Biofilm formation on stones causing chronic inflammation
C. Acute necrotizing cholecystitis
D. Pancreatic duct obstruction
Correct answer: B
-
Anomalous pancreaticobiliary junction predisposes to GBC because it:
A. Causes biliary atresia
B. Permits pancreatic enzyme reflux into the biliary tree
C. Blocks cystic duct emptying
D. Prevents gallstone formation
Correct answer: B
-
GBC shows a unique gastrointestinal cancer pattern of:
A. Male predominance with worse outcomes
B. Female predominance with ER/PR positivity linked to better prognosis
C. Equal sex distribution with no hormonal influence
D. Male predominance with ER/PR positivity linked to worse prognosis
Correct answer: B
-
The gallbladder’s absence of which layer critically influences early spread?
A. Mucosa
B. Muscularis
C. Submucosa
D. Serosa
Correct answer: C
-
T1a GBC is defined by invasion:
A. Into muscularis
B. Confined to lamina propria
C. Into perimuscular connective tissue
D. Through serosa
Correct answer: B
-
T1b GBC requires which operation?
A. Simple cholecystectomy only
B. Pancreaticoduodenectomy
C. Radical cholecystectomy with wedge of segments IVb and V and regional lymphadenectomy
D. Liver transplant
Correct answer: C
-
The primary initial imaging for suspected gallstones is:
A. MRI
B. Ultrasound
C. PET-CT
D. Plain radiograph
Correct answer: B
-
The cornerstone imaging modality for staging GBC is:
A. Contrast-enhanced CT
B. Ultrasound
C. PET-CT alone
D. Endoscopic ultrasound
Correct answer: A
-
MRI/MRCP is most helpful to:
A. Assess bone metastases
B. Map biliary ductal anatomy and involvement
C. Evaluate pulmonary metastases
D. Replace histopathology
Correct answer: B
-
Discovery of peritoneal carcinomatosis at exploration for GBC should lead to:
A. Extended resection to achieve R0
B. Ablation of all lesions
C. Abandoning curative resection and planning systemic therapy
D. Immediate transplant referral
Correct answer: C
-
After resection of GBC, recurrence rates may reach:
A. 10%
B. 30%
C. 50%
D. 70%
Correct answer: D
-
The ABCO2 trial established which standard for advanced biliary tract cancers?
A. Capecitabine monotherapy superiority
B. Gemcitabine–cisplatin superiority over gemcitabine alone
C. FOLFIRINOX superiority
D. Immunotherapy alone superiority
Correct answer: B
-
In the adjuvant setting after resection, the BILCAP trial supports:
A. Observation alone
B. Adjuvant capecitabine
C. Neoadjuvant radiation
D. EGFR inhibitor monotherapy
Correct answer: B
-
Chemoradiation (e.g., SWOG S0809) is particularly considered for:
A. R0 resections
B. T1a tumors
C. R1 resections
D. Patients without nodal disease
Correct answer: C
-
HER2 (ERBB2) in GBC is notable because:
A. It is absent in GBC
B. Amplification is less common than in cholangiocarcinoma
C. Amplification is relatively common and potentially actionable
D. Only predicts radioresistance
Correct answer: C
-
ELF3 frameshift mutations are important as they:
A. Confer platinum resistance
B. Create neoantigens amenable to peptide vaccine strategies
C. Inactivate mismatch repair uniformly in India
D. Eliminate need for surgery
Correct answer: B
-
A systems-level practice to improve GBC detection is to:
A. Reserve histopathology for visibly abnormal gallbladders only
B. Perform routine histopathology on all cholecystectomy specimens
C. Avoid imaging in biliary colic
D. Defer pathology to reduce costs
Correct answer: B
MOTIVATIONAL MESSAGE FROM DR. R. K. MISHRA:
“In surgery, precision begins long before the incision—discipline in diagnosis, staging, and planning is the first and most vital cut.”
Wishing each of you clarity in judgment, steadiness in technique, and unwavering commitment to patient safety as you refine your craft.
| Older Post | Home | Newer Post |





