BASIC INFORMATION
Date & Time: June 8, 2026, 20:25:39 Indian Standard Time
Lecture Handout Prepared from the Teaching Session by: Dr. R. K. Mishra
SUMMARY
This unified lecture presents a comprehensive, stepwise approach to the diagnosis and management of abdominal tuberculosis (TB), emphasizing its paucibacillary nature and the necessity of multimodal confirmation. Clinical suspicion is guided by chronic gastrointestinal symptoms, ascites, right iliac fossa masses, and subacute obstruction, particularly in endemic regions and immunocompromised patients. Imaging localizes disease and guides targeted tissue acquisition; however, imaging is never independently diagnostic. Endoscopy and image-guided techniques are used to obtain deep, high-quality tissue specimens. Definitive diagnosis integrates histopathology (caseating granulomas), nucleic acid amplification tests (NAT/GeneXpert), acid-fast bacilli (AFB) smear, and mycobacterial culture (including drug susceptibility testing). Management of drug-susceptible disease follows a standard six-month anti-tubercular therapy (ATT) regimen, with close clinical monitoring and prudent use of endoscopic or surgical intervention for complications such as fibrotic strictures, perforation, abscess, fistulae, and diagnostic uncertainty. Medicolegal emphasis is placed on ruling out TB before initiating immunosuppression for suspected inflammatory bowel disease and excluding malignancy in mass lesions.
KEY KNOWLEDGE POINTS
-
Abdominal TB is a paucibacillary disease; diagnosis requires a combined clinical, radiological, endoscopic, histopathological, and microbiological approach.
-
Imaging (ultrasound, CT/MR enterography, barium studies) is highly suggestive but not diagnostic; it guides localization and biopsy.
-
The ileocecal region is most commonly involved; characteristic endoscopic ulcers are transverse/circumferential.
-
Deep, targeted biopsies are essential; specimens must be submitted simultaneously for histopathology, NAT/GeneXpert, AFB smear, and mycobacterial culture (solid and liquid media).
-
Caseating granulomas favor TB; small non-caseating granulomas suggest Crohn’s disease; suppurative granulomas may indicate Yersinia infection.
-
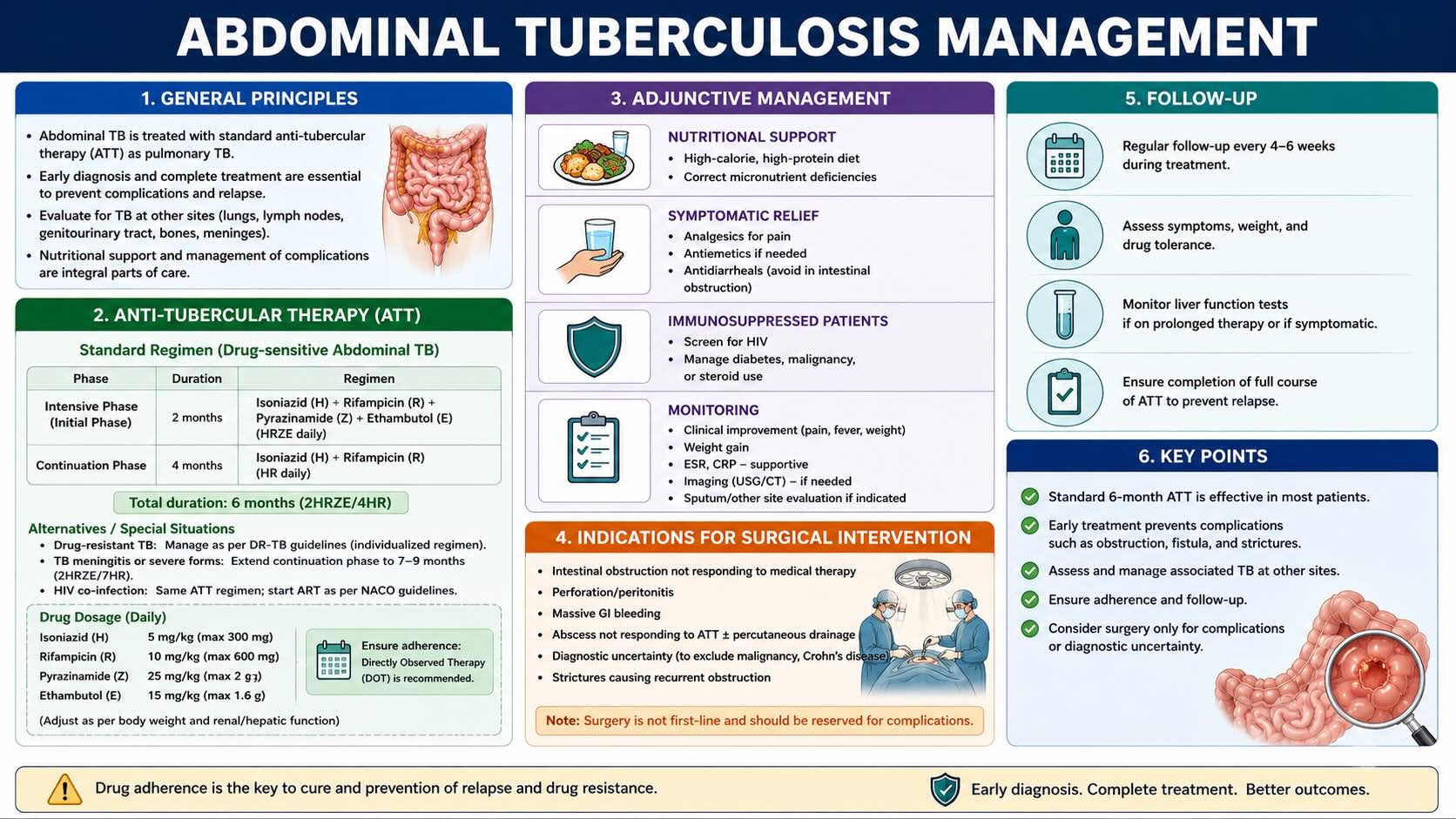
Standard ATT for drug-susceptible abdominal TB is six months (HRZE for two months, then HR for four months).
-
Surgical intervention is reserved for obstruction (especially fibrotic strictures), perforation, abscess/fistulae, and unresolved diagnostic uncertainty.
-
Steroids must be avoided until TB is definitively excluded; malignancy must be excluded before empirical ATT in mass lesions.
-
Negative NAAT, AFB smear, or culture does not exclude TB in high-suspicion cases.
INTRODUCTION
Abdominal tuberculosis remains a significant diagnostic and therapeutic challenge in endemic regions and among immunocompromised populations. Its protean manifestations mimic Crohn’s disease, gastrointestinal malignancies, and other granulomatous conditions, rendering reliance on any single modality unsafe. Low bacillary load in tissue and fluid (paucibacillary state) reduces test sensitivity, necessitating a structured, multimodal strategy. Accurate diagnosis hinges on clinical vigilance, imaging-guided localization, deep targeted biopsies, and concurrent histopathological and microbiological confirmation. Evidence-based management using standard ATT, careful monitoring, and judicious surgical intervention prevents complications, avoids inappropriate immunosuppression, and mitigates medicolegal risk.
LEARNING OBJECTIVES
-
Recognize clinical scenarios that warrant high suspicion for abdominal TB and understand the limitations and strengths of imaging modalities.
-
Apply systematic endoscopic and image-guided biopsy strategies and process specimens for histopathology, NAT/GeneXpert, AFB smear, and culture.
-
Formulate management plans including standard ATT, monitoring response, and indications for surgical intervention in complicated disease.
CORE CONTENT
1. Diagnostic Principles and Strategy
Abdominal TB is inherently difficult to diagnose because of its paucibacillary nature. The diagnostic process is sequential:
-
High clinical suspicion based on symptoms, endemicity, and risk factors.
-
Imaging to localize pathology and plan tissue acquisition.
-
Targeted collection of high-quality tissue/fluid specimens.
-
Concurrent laboratory investigations: histopathology, NAT/GeneXpert, AFB smear, and mycobacterial culture (with drug susceptibility testing).
1.1 Clinical Suspicion: Indications
-
Chronic abdominal pain, weight loss, low-grade fever, night sweats.
-
Right iliac fossa pain/mass; differential includes cecal carcinoma.
-
Recurrent subacute intestinal obstruction: colicky pain, vomiting, distension.
-
Exudative ascites suggestive of peritoneal involvement.
-
Systemic symptoms with pancreatic or cecal masses on imaging; malignancy must be excluded but TB considered strongly.
-
Crohn’s disease-like phenotype in endemic areas before initiating biologics; misdiagnosis risks disseminated TB.
-
High-risk groups: immunocompromised, diabetic, or on immunosuppressive therapy.
1.2 Role of Imaging
Imaging localizes disease and guides biopsy; it is not diagnostic on its own.
-
Ultrasound: bowel wall thickening (ileocecal), mesenteric lymphadenopathy (often necrotic), peritoneal thickening, loculated ascites, solid organ lesions; pseudo-kidney sign of the cecum.
-
CT/MR enterography: preferred for comprehensive evaluation of bowel enhancement, mural thickening, annular strictures, proximal dilatation, rim-enhancing necrotic nodes, ascites, peritoneal/omental thickening, solid organ lesions.
-
Barium studies: inverted umbrella (Fleischner) sign; goose neck appearance; obtuse ileocecal angle; filling defects/strictures; herringbone pattern with proximal ileal dilatation and hypersegmentation; pulled-up cecum.
2. Endoscopy and Targeted Tissue Acquisition
2.1 Indications and Endoscopic Findings
-
Ileocolonoscopy indicated when imaging suggests ileocecal involvement.
-
Findings: ulcers at ileocecal valve/cecum; transverse or circumferential (girdle-type) ulcers; nodules surrounding ulcers; mucosal thickening; stricture formation; pseudopolyps.
-
Longitudinal ulcers are more typical of Crohn’s disease.
2.2 Biopsy Technique and Rationale
-
Obtain deep biopsies from ulcer edges and bases, ileocecal valve nodules, cecal nodules, and surrounding mucosa.
-
Granulomas in intestinal TB are submucosal/deeper; superficial biopsies risk false negatives.
3. Specimen Processing and Laboratory Confirmation
Submit all specimens simultaneously:
-
Histopathology: evaluate granuloma size/distribution; caseation necrosis; AFB staining. Large confluent caseating granulomas suggest TB; small non-caseating granulomas suggest Crohn’s disease; suppurative granulomas raise suspicion for Yersinia.
-
NAT/GeneXpert: rapid detection of mycobacterial DNA and rifampicin resistance; sensitivity limited in paucibacillary disease; a negative test does not exclude TB.
-
AFB smear: rapid but low sensitivity in abdominal TB; positive results are specific.
-
Mycobacterial culture: microbiological gold standard; perform on solid and liquid media; essential for drug susceptibility testing; slow turnaround and potentially low yield due to low bacillary load.
4. Site-Directed Specimen Acquisition
-
Intestinal disease: colonoscopy with deep biopsies of ulcers, nodules, ileocecal valve, and cecum.
-
Peritoneal disease with ascites: ascitic fluid analysis (cell count, biochemistry, cytology, NAT, culture); if non-diagnostic, diagnostic laparoscopy with targeted peritoneal biopsy.
-
Lymphadenopathy: ultrasound/CT-guided or endoscopic ultrasound-guided FNA/core biopsy of mesenteric/retroperitoneal nodes.
-
Hepatic/splenic/pancreatic lesions: image-guided biopsy; EUS-FNA/FNB for pancreatic/peripancreatic lesions.
-
Persistent uncertainty: laparoscopic peritoneal biopsy.
5. Differential Diagnosis and Interpretation of Findings
-
Strong diagnostic evidence for TB: imaging/endoscopic features consistent with ileocecal TB plus histopathological caseating granulomas combined with positive NAT/GeneXpert or culture.
-
Exclude malignancy in all mass lesion presentations before starting ATT.
-
Avoid corticosteroids until TB is confirmed or conclusively excluded to prevent dissemination.
6. Medical Management: Anti-Tubercular Therapy (ATT)
6.1 Standard Regimen for Drug-Susceptible Disease
-
Intensive phase (first 2 months): Isoniazid (H), Rifampicin (R), Pyrazinamide (Z), Ethambutol (E).
-
Continuation phase (next 4 months): Isoniazid (H), Rifampicin (R).
-
Obtain drug susceptibility testing (DST) via culture or molecular methods on initial biopsy specimens; modify regimen for resistance.
6.2 Monitoring Treatment Response
-
Clinical assessment at 4–8 weeks: improvement in constitutional symptoms, weight gain, appetite recovery, resolution of abdominal pain/altered bowel habits.
-
Lack of improvement by 8 weeks: reassess for incorrect diagnosis (Crohn’s, malignancy, lymphoma), drug resistance, non-adherence, or complications (e.g., fibrotic stricture/abscess).
-
Imaging/endoscopy reserved for poor response, complications, or diagnostic uncertainty; routine repeat studies are unnecessary in responders.
-
Microbiological follow-up is limited in utility due to paucibacillary disease.
6.3 Pre-Treatment Evaluation
-
Baseline LFTs and RFTs; viral serology (Hepatitis B/C); pregnancy test where appropriate; thorough drug history for interactions.
7. Pathophysiology and Management of Tuberculous Intestinal Strictures
-
Inflammatory (edematous) strictures: early, potentially reversible; respond to ATT.
-
Fibrotic strictures: late, irreversible scarring; do not respond to ATT; often need endoscopic balloon dilatation or surgery.
-
Mixed strictures: inflammatory component improves with ATT, residual fibrosis may cause persistent obstruction.
-
Endoscopic balloon dilatation: suitable for short, accessible fibrotic strictures after 4–8 weeks of effective ATT with surgical backup.
-
Surgical options: strictureplasty, limited resection, intestinal bypass for long/multiple strictures or failed endoscopic therapy.
8. Indications for Surgical Intervention
-
Diagnostic uncertainty: laparoscopy with targeted biopsy when noninvasive methods fail.
-
Intestinal obstruction: acute complete obstruction or refractory subacute obstruction due to fibrotic strictures.
-
Perforation: emergency laparotomy, resection of perforated segment, peritoneal lavage.
-
Abscess formation: percutaneous drainage under imaging guidance for large intra-abdominal or psoas abscesses; surgical drainage if not amenable to percutaneous techniques.
-
Fistulae: entero-enteric, enterocutaneous, or complex fistulae may require surgical resection.
-
Massive hemorrhage: rare; may necessitate emergency surgery.
-
Abdominal cocoon (sclerosing encapsulating peritonitis): extensive adhesiolysis.
9. Anesthetic and Physiological Considerations
Not specifically discussed in the lecture.
10. Complications and Their Management
-
Intraoperative: difficulty obtaining deep tissue endoscopically due to strictures/friability; consider image-guided or laparoscopic biopsy. Perforation or bleeding during deep endoscopic biopsy or dilatation requires immediate standard endoscopic hemostasis or conversion to surgery.
-
Early postoperative: wound infection, anastomotic leak, prolonged ileus; manage per standard surgical protocols.
-
Late postoperative: recurrent stricture formation, adhesive small bowel obstruction; investigate and manage with re-intervention as needed.
-
Medical complication (drug-induced liver injury, DILI): if LFTs >5× ULN, or >3× ULN with symptoms/elevated bilirubin, stop all hepatotoxic ATT drugs; reintroduce sequentially per established protocols.
11. Medicolegal and Patient Selection Considerations
-
Do not base diagnosis solely on imaging or a single test; document multimodal evaluation.
-
Exclude malignancy histopathologically in mass lesions before initiating ATT.
-
Avoid corticosteroids until TB is confirmed or excluded; steroids in undiagnosed TB risk dissemination and carry medicolegal implications.
-
Perform and document DST to guide therapy and demonstrate evidence-based management.
-
Maintain a lower threshold for investigation in immunocompromised patients (HIV, diabetes, immunosuppressants).
-
Never start biologic therapy for suspected IBD in endemic areas without definitively ruling out TB, preferably via tissue diagnosis.
SURGICAL PEARLS
-
Deep biopsies are mandatory in suspected intestinal TB; superficial samples often miss submucosal granulomas.
-
Submit all specimens concurrently for histopathology, AFB smear, NAT/GeneXpert, and culture to maximize yield and avoid delays.
-
Girdle-type circumferential ulcers favor TB over Crohn’s disease; longitudinal ulcers suggest Crohn’s.
-
Consider image-guided node biopsy for necrotic lymphadenopathy identified on imaging.
-
Repeat biopsy with deeper or image-guided technique if initial colonic biopsy is negative but suspicion remains high.
-
Healing in TB may involve fibrosis; counsel patients regarding potential worsening of strictures during therapy and possible need for intervention.
-
Do not initiate corticosteroids until TB is excluded; avoid medicolegal pitfalls by thorough documentation and evidence-based decisions.
ANESTHETIC AND PHYSIOLOGICAL CONSIDERATIONS
-
Not addressed in this lecture.
COMPLICATIONS AND THEIR MANAGEMENT
-
Intraoperative:
-
Bleeding or perforation during deep endoscopic biopsy or dilatation: apply endoscopic hemostasis; convert to surgery if required.
-
Difficulty attaining adequate deep tissue: switch to image-guided or laparoscopic biopsy.
-
-
Early postoperative:
-
Wound infection, anastomotic leak, prolonged ileus: manage per standard surgical care pathways.
-
-
Late postoperative:
-
Recurrent strictures; adhesive small bowel obstruction: evaluate and consider endoscopic/surgical re-intervention.
-
-
Medical:
-
Drug-induced liver injury: stop hepatotoxic agents when thresholds are met; reintroduce sequentially under protocol.
-
MEDICOLEGAL AND PATIENT SELECTION CONSIDERATIONS
-
Multimodal diagnostic confirmation is essential; never rely on a single negative test to exclude TB in high-suspicion contexts.
-
Exclude malignancy prior to empirical ATT in mass lesions.
-
Avoid steroids and biologics until TB is excluded; misdiagnosis leading to immunosuppression in active TB has grave clinical and legal consequences.
-
Document DST and tailored therapy; ensure informed consent regarding treatment duration, hepatotoxicity risks, and potential need for surgery.
-
Prioritize definitive tissue diagnosis to prevent mismanagement of Crohn’s disease and malignancy.
SUMMARY AND TAKE-HOME MESSAGES
-
Abdominal TB requires a sequential, multimodal diagnostic approach; imaging is suggestive but not diagnostic.
-
Deep, high-quality biopsies with simultaneous histopathology, NAT/GeneXpert, AFB smear, and culture maximize diagnostic yield; caseating granulomas with NAT/culture positivity provide strong evidence.
-
Standard six-month ATT is effective for drug-susceptible disease; monitor clinically and reserve imaging/endoscopy for poor response or complications; use endoscopic or surgical interventions for fibrotic strictures, perforation, abscess, fistulae, or unresolved diagnostic uncertainty.
MULTIPLE CHOICE QUESTIONS (MCQs)
-
Which principle best characterizes the diagnostic role of imaging in abdominal TB?
a) Imaging alone is diagnostic
b) Imaging is highly suggestive but not independently diagnostic
c) Imaging is unnecessary
d) Imaging replaces biopsy
Correct answer: b
-
The most common intestinal site involved in abdominal TB is:
a) Duodenum
b) Jejunum
c) Ileocecal region
d) Sigmoid colon
Correct answer: c
-
The inverted umbrella (Fleischner) sign on barium study reflects:
a) Longitudinal colonic ulcers
b) Narrowing of the terminal ileum with thickening
c) Cecal perforation
d) Diffuse colonic dilatation
Correct answer: b
-
A characteristic CT feature of abdominal TB lymphadenopathy is:
a) Homogeneous enhancement of nodes
b) Rim-enhancing necrotic nodes
c) Calcified nodes only
d) Absence of lymphadenopathy
Correct answer: b
-
The endoscopic ulcer pattern favoring intestinal TB over Crohn’s disease is:
a) Longitudinal aphthous ulcers
b) Transverse/circumferential (girdle-type) ulcers
c) Cobblestoning without ulcers
d) No ulceration
Correct answer: b
-
Deep biopsies are required in suspected intestinal TB because:
a) Superficial biopsies are technically difficult
b) Granulomas are submucosal or deeper
c) Deep biopsies are painless
d) Superficial biopsies always bleed
Correct answer: b
-
Which statement about NAT/GeneXpert in abdominal TB is correct?
a) A negative result excludes TB
b) It rapidly detects mycobacterial DNA and rifampicin resistance
c) It replaces histopathology
d) It is slower than culture
Correct answer: b
-
The microbiological gold standard for confirming TB and obtaining DST is:
a) Histopathology
b) AFB smear
c) Mycobacterial culture on solid and liquid media
d) Serum antibody test
Correct answer: c
-
In peritoneal TB with non-diagnostic ascitic analysis, the next best step is:
a) Empirical ATT
b) Repeat tap after one week
c) Diagnostic laparoscopy with targeted peritoneal biopsy
d) Chest X-ray
Correct answer: c
-
A histopathological feature strongly supporting TB over Crohn’s disease is:
a) Any granuloma
b) Large confluent caseating granulomas
c) Non-caseating microgranulomas
d) Villous atrophy
Correct answer: b
-
Suppurative granulomas in ileocecal biopsies should prompt consideration of:
a) Ulcerative colitis
b) Yersinia enterocolitica infection
c) Ischemic colitis
d) Celiac disease
Correct answer: b
-
Which ultrasound finding is NOT typical of abdominal TB?
a) Bowel wall thickening
b) Ascites
c) Large simple renal cyst
d) Mesenteric lymphadenopathy
Correct answer: c
-
A core principle before initiating steroids for suspected Crohn’s disease in endemic areas is:
a) Start steroids first, then test for TB
b) Definitively exclude TB, preferably with tissue diagnosis
c) Rely on chest imaging alone
d) Check ESR only
Correct answer: b
-
The standard intensive phase of ATT for drug-susceptible abdominal TB is:
a) HR for 2 months
b) HRZ for 2 months
c) HRZE for 2 months
d) HRE for 2 months
Correct answer: c
-
The continuation phase of standard ATT consists of:
a) Isoniazid and Ethambutol
b) Isoniazid and Rifampicin
c) Rifampicin and Pyrazinamide
d) Rifampicin and Ethambutol
Correct answer: b
-
The primary reason fibrotic strictures respond poorly to ATT is:
a) Drug resistance
b) Acellular scar tissue causing irreversible narrowing
c) Poor drug absorption
d) Suboptimal dosing
Correct answer: b
-
In a patient with negative initial colonic biopsy but persistent high suspicion for intestinal TB, the most appropriate next step is:
a) Diagnose Crohn’s disease and start steroids
b) Repeat with deeper or image-guided biopsies
c) Discharge
d) Begin biologic therapy
Correct answer: b
-
The herringbone pattern on barium follow-through in abdominal TB is associated with:
a) Gastric outlet obstruction
b) Hypersegmentation with proximal ileal dilatation and partial obstruction
c) Colonic diverticulosis
d) Rectal involvement
Correct answer: b
-
Optimal management for a large intra-abdominal or psoas abscess in intestinal TB is:
a) ATT alone
b) Surgical drainage only
c) Image-guided percutaneous drainage combined with ATT
d) Six weeks of non-TB antibiotics
Correct answer: c
-
In suspected abdominal TB with a mass lesion, the mandatory step before starting ATT is:
a) Empirical treatment for four weeks
b) Histopathological exclusion of malignancy
c) Serologic testing for IBD
d) Immediate laparotomy
Correct answer: b
MOTIVATIONAL MESSAGE FROM DR. R. K. MISHRA
“Precision in diagnosis is the surgeon’s first operation—performed with thought, evidence, and restraint. Master it, and your hands will follow with clarity.”
May your pursuit of surgical excellence be steady and disciplined, and may every patient benefit from your diligence and compassion. My best wishes to all postgraduate surgeons and gynecologists in your continued learning and practice.
| Older Post | Home | Newer Post |





