Laparoscopic Palmer’s Access Technique
This access was advocated by Palmer in the 1940s because visceral parietal adhesions are rarely encountered in this area. A small incision is made to allow the insertion of the Veress needle through the left subcostal margin. In addition, some authors feel that because the abdominal wall in the area is supported by the rigid thoracic wall, the insertion of the needle is more controlled than in the periumbilical area. Palmer’s technique is particularly useful in cases where umbilical entry is contraindicated, it is preferred to use the left upper quadrate for entry of Veress needle. The Veress needle is introduced through left hypochondria, i.e. Palmer’s point 2 cm below the left subcostal margin in the midclavicular line. Special care should be taken that there should not be hepatosplenomegaly. After access through the palmer’s point, the umbilicus site is re-checked for any adhesion or other abnormalities. If necessary, the umbilicus port may be introduced under vision.
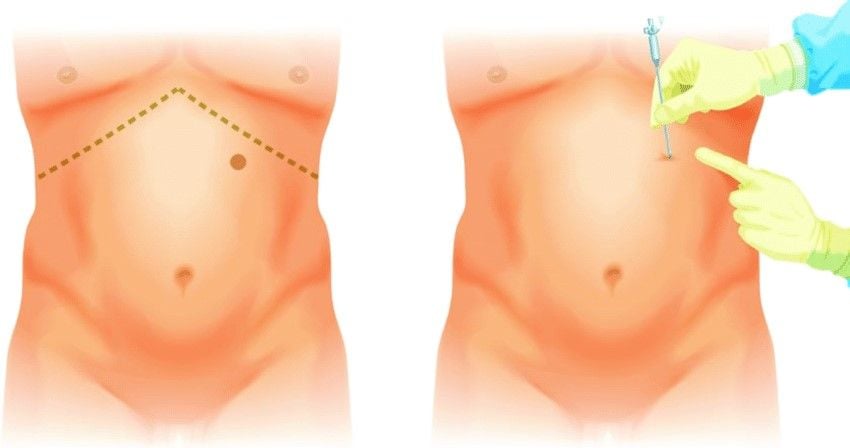
Palmer’s point of access
Palmer’s point 2 cm below the costal margin

Veress Needle insertion through Palmer’s Point
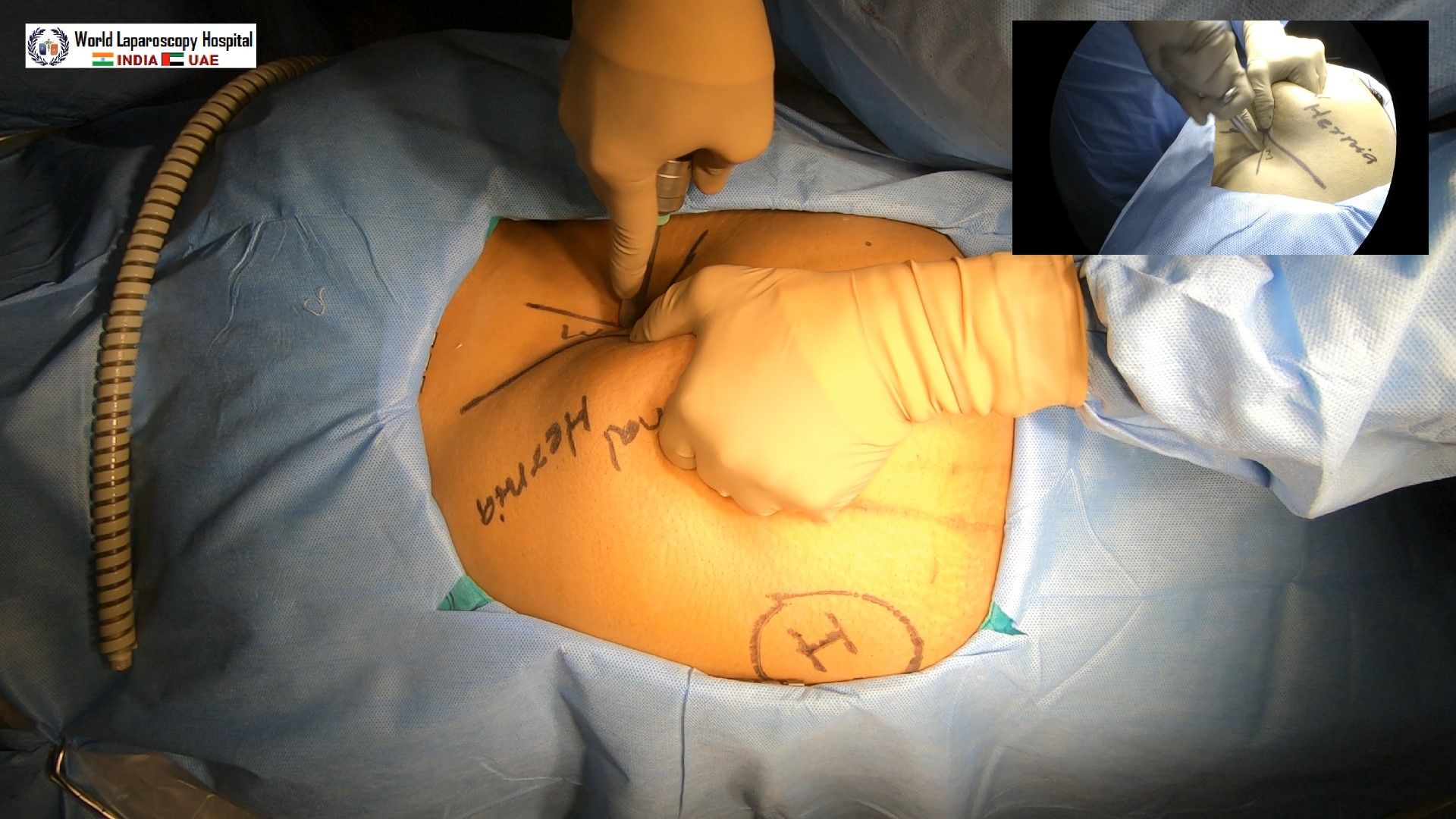
Mishra’s Technique
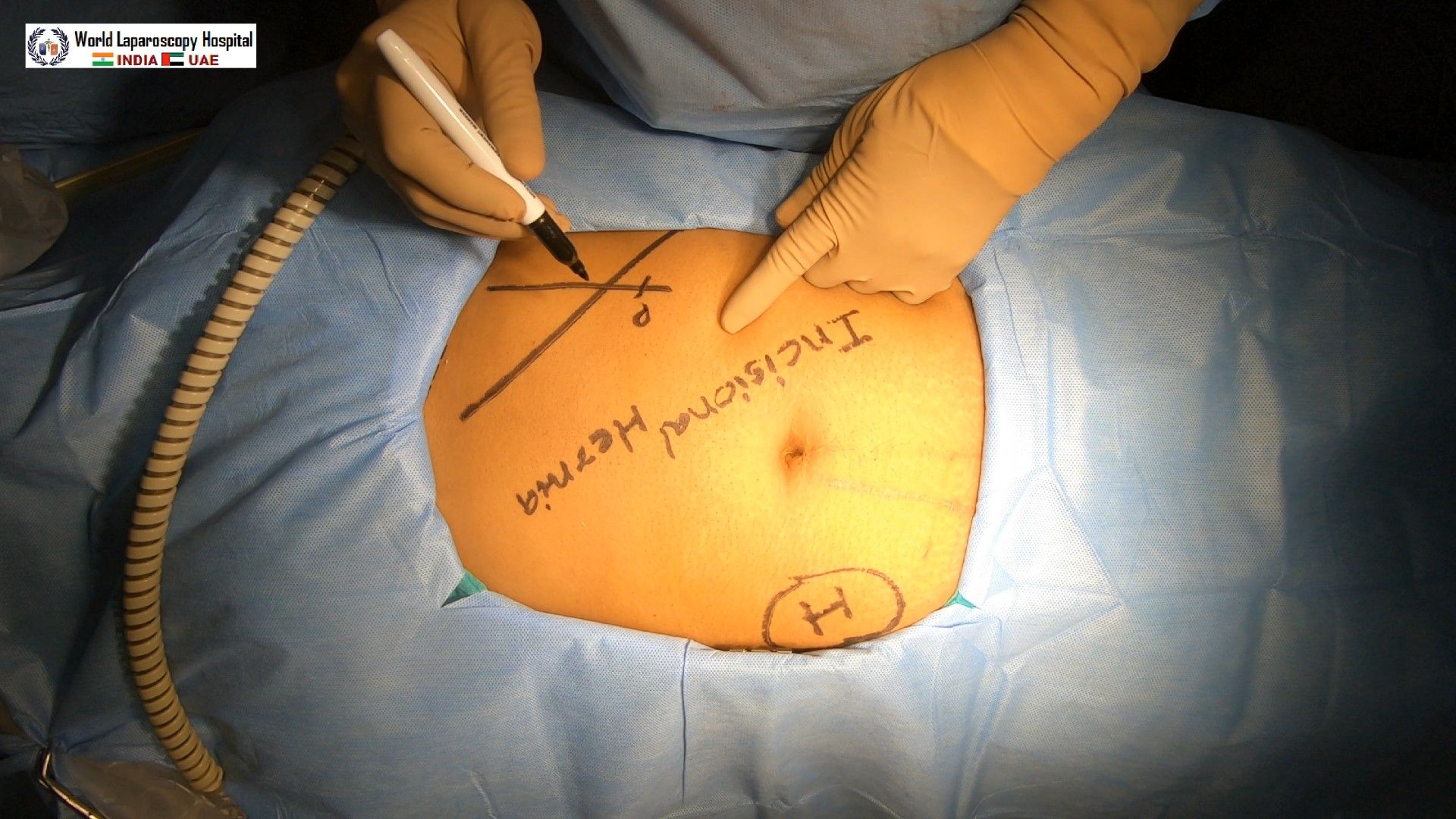
This access technique we have developed where little modification of Palmer’s technique is done. We give incision 2 cm above the costal margin in the midclavicular line called Mishra’s Point. To introduce a Veress needle at Mishra’s point abdominal wall is stretched down and brought below the costal margin. The advantage of this technique is there is no incidence of hernia because after surgery incision retracts back to 2 cm above the costal margin. During the insertion of the Veress need or trocar through the Palmer’s Point, the tip of the trocar should be pointed towards the stomach to prevent injury of splenic flexor of the colon. It is very important that a nasogastric tube should be in place and the stomach should be deflated.
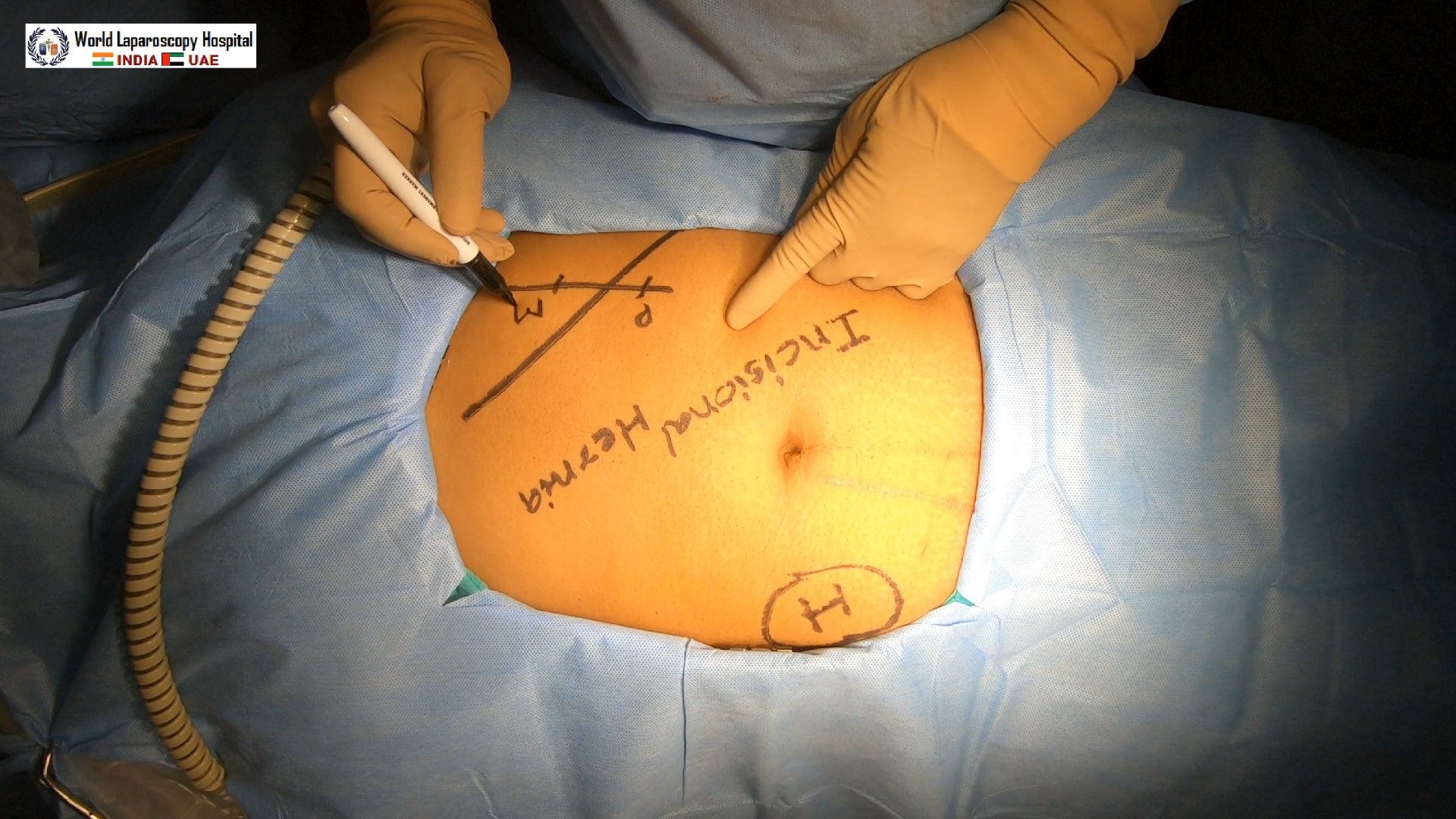
Mishra’s point 2 Cm above the costal margin
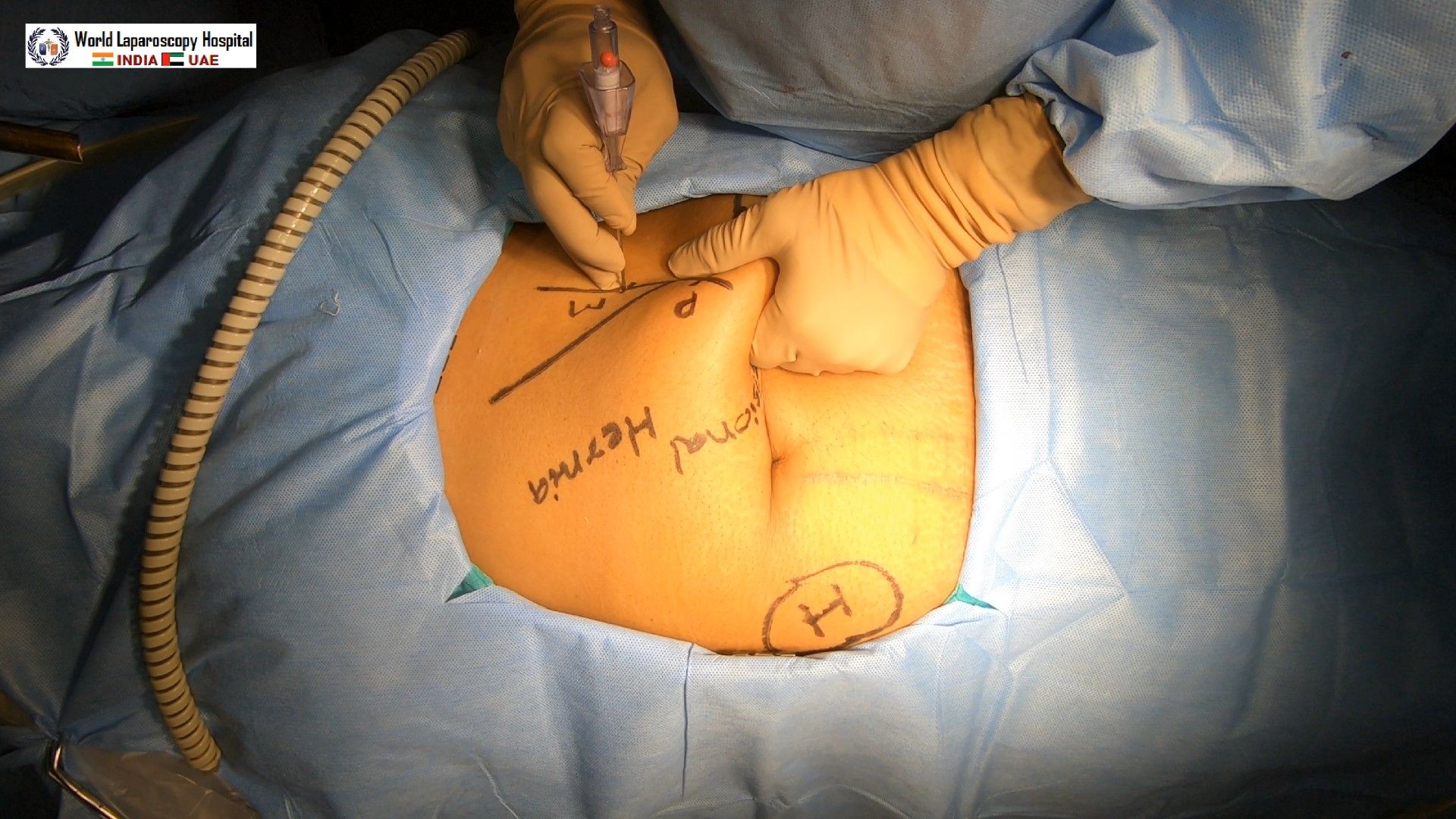
Veress Needle insertion through Mishra’s Point
Trocar insertion through Mishra’s Point
Mishra's point has demonstrated no hernia postoperatively in 150 cases performed in the last 10 years of study. Post closure was not done in any of the patients.
This access was advocated by Palmer in the 1940s because visceral parietal adhesions are rarely encountered in this area. A small incision is made to allow the insertion of the Veress needle through the left subcostal margin. In addition, some authors feel that because the abdominal wall in the area is supported by the rigid thoracic wall, the insertion of the needle is more controlled than in the periumbilical area. Palmer’s technique is particularly useful in cases where umbilical entry is contraindicated, it is preferred to use the left upper quadrate for entry of Veress needle. The Veress needle is introduced through left hypochondria, i.e. Palmer’s point 2 cm below the left subcostal margin in the midclavicular line. Special care should be taken that there should not be hepatosplenomegaly. After access through the palmer’s point, the umbilicus site is re-checked for any adhesion or other abnormalities. If necessary, the umbilicus port may be introduced under vision.
Palmer’s point of access
Palmer’s point 2 cm below the costal margin
Veress Needle insertion through Palmer’s Point
Mishra’s Technique
This access technique we have developed where little modification of Palmer’s technique is done. We give incision 2 cm above the costal margin in the midclavicular line called Mishra’s Point. To introduce a Veress needle at Mishra’s point abdominal wall is stretched down and brought below the costal margin. The advantage of this technique is there is no incidence of hernia because after surgery incision retracts back to 2 cm above the costal margin. During the insertion of the Veress need or trocar through the Palmer’s Point, the tip of the trocar should be pointed towards the stomach to prevent injury of splenic flexor of the colon. It is very important that a nasogastric tube should be in place and the stomach should be deflated.
Mishra’s point 2 Cm above the costal margin
Veress Needle insertion through Mishra’s Point
Trocar insertion through Mishra’s Point
Mishra's point has demonstrated no hernia postoperatively in 150 cases performed in the last 10 years of study. Post closure was not done in any of the patients.





