Laparoscopic Salpingectomy for Women with Hydrosalpinges
Laparoscopic Salpingectomy means the surgical removal of Fallopian tube using laparoscopic technique. It is often performed in cases of ectopic pregnancies in the fallopian tubes. Removal of the fallopian tubes is preferred over other procedures which don’t involve its removal because of the high rate of recurrence in ectopic pregnancies related to the Fallopian tubes. The most common indication for the procedure of salpingectomy is in cases of ectopic pregnancy but it can also be performed in cases of inflammatory disease with unilateral hydrosalpinx.
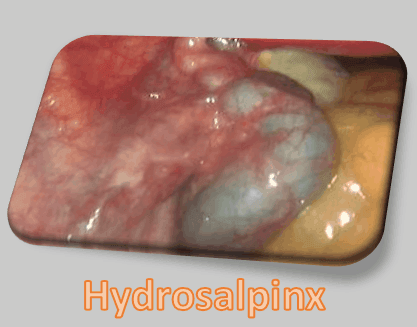
In vitro fertilization (IVF) is commonly used for treating infertility caused by tubal disease. IVF is the only treatment for damaged, inoperable fallopian tubes. Hydrosalpinx (or fallopian tube obstruction) refers to a tubal disease in which there is fluid filled distension of the fallopian tube with distal tubal occlusion. It can involve either the proximal, distal or the whole fallopian tube. The distal tubal occlusion is usually a result of pelvic inflammatory diseases (PID) which causes severe inflammation obstructing the distal end of the fallopian tube. The inflammatory response together with transitional cell mucosa production produce swollen non-functioning hydrosalpinx fluid. Hydrosalpinx is classified according to severity of damage to the fallopian tubes into:
- grade I (Mild)
- grade II (Moderate)
- grade III (Severe)
Hydrosalpinx is a leading cause of female infertility.
Objective
The objective of Laparoscopic salpingectomy is to remove the Fallopian tube such that the uterus and ovary remain intact.
Precautions
Hemostasis must be provided as the cornual portion of the Fallopian tube and mesosalpinx are highly vascular.
Technique
- Positioning: the patient is positioned in the lithotomy position which can be modified to conform to the specific requirements of the procedure.
- The legs are positioned at 45� flexion from the hip.
- The buttocks should be positioned at least 4 inches off the end of the operating table to help in usage of the cervical and intrauterine instruments for better visualization of the genitalia.
- The operating table is angulated at a 15� Trendelenburg position such that the intestines are into the upper abdomen.
- Anaesthesia: general anaesthesia is administered by the standard techniques used for major abdominal operations.
- A bimanual pelvic examination is performed prior to the laparoscopy procedure.
Main Laparoscopic Operatice Procedure:
- A laparotomy is performed either via a transverse or midline incision. All peritubal adhesions are relieved from the diseased fallopian tube.
- Using a Kelly clamp the cornual portion of the tube is clamped and the remaining portion is grasped with a Babcock clamp and elevated to a comfortable position.
- Repeated fenestrations are made in the mesosalpinx using a straight Halsted clamp which are then clamped between small hemostats. The tube is then excised from the cornual portion across the mesosalpinx to the fimbria.
- Each �pedicle of the hemostat is tied with an interrupted 3-0 synthetic absorbable suture.
- After re-establishing the peritoneal lining, the cornual portion of the tube is buried with an interrupted 3-0 mattress suture in the broad ligament to the posterior portion of uterine cornu.
- The mesosalpinx is also reperitonealized with a 3-0 synthetic absorbable suture.
- The mesosalpinx is then closed with a running 3-0 synthetic absorbable suture. The abdomen is closed in routine fashion. This completes the procedure.
Prognosis
The cause of tubal disease must be considered when determining the prognosis for any surgical procedure. Successful results will depend on whether the cause of tubal disease is because of intrinsic factors or extrinsic causes.
Advantages
Studies have shown that women with hydrosalpinges who undergo Laparoscopic salpingectomy before undergo IVF have higher chances of pregnancy and live birth to babies. Though further research is also required to assess effectiveness of other pre-IVF surgical procedures like needle aspiration of hydrosalpinx fluid, laparoscopic proximal tubal occlusion and laparoscopic salpingostomy for women with hydrosalpinges.
For more information:
World Laparoscopy Hospital, Cyber City, DLF Phase II, Gurugram, NCR Delhi, 122 002, India
PHONES:
For Training: +919811416838
For Treatment: +919811912768
For General Enquiry: +91(0)124 - 2351555
Email: contact@laparoscopyhospital.com





