Video of Laparoscopic Cholecystectomy. To download video right click here and save target
Download video of Laparoscopic Cholecystectomy
Laparoscopic cholecystectomy is now the gold standard for the treatment of symptomatic gallstone disease. It is most commonly performed Minimal Access Surgery by General surgeon's world wide. In Europe and America 98% of all the cholecystectomy is performed by laparoscopy.
Common Indications are:
- Cholelithiasis
- Mucocele gall bladder
- Empyema ball bladder
- Cholesterosis
- Typhoid carrier
- Porcelain gallbladder
- Acute Cholecystitis (calculous and acalculous)
- Adenomatous gall bladder polyps
- As part of other procedures viz. Whipple's procedure
Advantage of laparoscopic approach:
- Cosmetically better outcome.
- Less tissue dissection and disruption of tissue planes
- Less pain postoperatively.
- Low intra-operatively and postoperative complications.
- Early return to work.
Pre-operative Investigations:
Apart from routine pre-operative investigations, in fit patients, the only investigations needed are ultrasound examination, although practiced in some centers; intravenous Cholangiography may not be confirmative and is attended with the risk of anaphylactic reactions.
Relative contra-indications:
- Complicated Cholecystitis.
- Poor risk for general anaesthesia.
- Some cases of previous extensive abdominal surgery.
The general anaesthesia and the pneumoperitoneum required as part of the laparoscopic procedure do increase the risk in certain groups of patients. Most surgeons would not recommend laparoscopy in those with pre-existing disease conditions. Patients with severe cardiac diseases and COPD should not be considered a good candidate for laparoscopy. The laparoscopic cholecystectomy may also be more difficult in patients who have had previous upper abdominal surgery. The elderly may also be at increased risk for complications with general anaesthesia combined with pneumoperitoneum.
Patient position
Patient is operated in the supine position with a steep head-up and left tilt once the pneumoperitoneum has been established.
Position of Surgical team
The surgeon stands on the left side of the patient with the scrub nurse-camera holder-assistant. One assistant stand right to the patient and he will hold the fundus grasping forceps.
Tasks analysis
- Preparation of the patient.
- Creation of pneumoperitoneum.
- Insertion of ports
- Diagnostic laparoscopy
- Dissection of visceral peritoneum
- Dissection of Calot's triangle
- Clipping and division of cystic duct and artery
- Dissection of gallbladder from liver bed.
- Extraction of gallbladder and any spilled stone.
- Irrigation and suction of operating field.
- Final Diagnostic laparoscopy.
- Removal of the instrument with complete exit of CO2.
- Closure of wound.
Port location
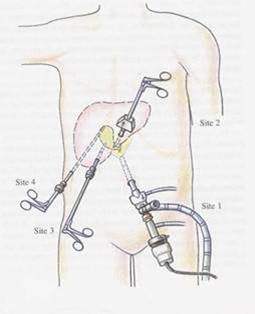
Four ports are used: optical (10mm), one 5mm and one 10mm operating, and one 5.0mm assisting port. The optical port is at or near the umbilicus and routinely a 30� laparoscope is used. Some surgeon who has started laparoscopy earlier they are more comfortable with 0 degree telescope.
First view of gallbladder after insertion of telescope
Once all the four ports are in position the fundus of the gallbladder is grasped by the assistant and flipped upwards and over the superior edge of the right lobe of liver.
Dissection of Cystic Pedicle
Any adhesion should be cleared from the gallladder. Sharp dissection may be carried out with the help of scissors attached with monopolar current. At the time of separating adhesion surgeon should try to be as near as possible towards gallbladder. The cystic pedicle is a triangular fold of peritoneum containing the cystic duct and artery, the cystic node and a variable amount of fat. It has a superior and an inferior leaf which are continuous over the anterior edge formed by the cystic duct. An important consideration is the frequent anomalies of the structures contained between the two leaves (15 -20%). The normal configuration is for an anterior cystic duct with the cystic artery situated postero-superiorly and arising from the right hepatic artery usually behind the common bile duct.
Pledget dissection of Cystic pedicle
The dissection of the cystic pedicle can be carried out with two handed technique. The dissection should be started with antero-medial traction by left hand grasper placed on the anterior edge of Hartmann's pouch, The antero-medial traction by left hand will expose the posterior peritoneum. The peritoneum of the posterior leaf of the cystic pedicle is divided superficially as far back as the liver. Posterior leaf is better to dissect before anterior leaf because it is relatively less vascular & the bleeding if any, will not soil the anterior peritoneum, whereas if anterior peritoneum is tackled first it my make the dissection area of posterior peritoneum filled with blood making dissection of this area difficult. Once the visceral peritoneum is dissected a pledget mounted securely in a pledget holder is used for blunt dissection.
Separation of Cystic artery from Cystic duct
The separation of the cystic duct anteriorly from the cystic artery behind can be performed by a Maryland's grasper by gently opening the jaw of Maryland between the duct and artery. The opening of the jaw of Maryland dissector should be in the line of duct never at right angle to avoid injury of artery behind. Sufficient length of the cystic duct and artery on the gallbladder side should be mobilised so that three clips can be applied.
Clipping of cystic artery
The cystic artery is clipped and then divided by hook scissors. Two clips are placed proximally on the cystic artery and one clip is applied distally. The artery is then grasped with a duckbill grasper on the gallbladder wall and then divided between second and third clip.
The dissection of the cystic pedicle is completed by placement of a clip to occlude the cystic duct at its junction with the gallbladder.
Operative Cholangiogram

In many institutions routine operative cholangiogram is performed. Routine cholangiogram decreases the risk of CBD injury in case of difficult anatomy. The opening in the cystic duct in made on the antero-superior aspect. Correct alignment of the cystic duct and infusion of saline facilitates insertion of ureteric catheter to perform cholangiography. Insertion is difficult if the opening in the cystic duct is made too close to the gallbladder. The contrast medium should be injected slowly during screening and the patient should be in a slight trendelenberg position with the table rotated slightly to the right. It is essential that the entire biliary tract is outlined. Surgeon should ligate or clip cystic duct when you are sure up to the point of absolute certainness.
Ligation of Cystic Duct
Although the majority of surgeons opt for clipping the cystic duct, before dividing it, this technique though quick is intrinsically unsound as internalisation of the metal clip inside the common bile duct over the ensuing months is well documented. There is report of internalization of clip and subsequent stone formation after many years. The internalised clip becomes covered with calcium bilirubinate pigment. For this reason, to tie the cystic duct using a catgut Roeder external slip knot should be done.
Dissection of Gallbladder from Liver Bed

Gallbladder should be seperated from the liver through the areolar tissue plane binding the gallbladder to the Glisson's capsule lining the liver bed. The actual separation can be performed with scissors with electrosurgical attachment or electrosurgical hook knife. Pledget can be used to remove the gallbladder from liver bed once a good plane of dissection is found. Perforation of the gallbladder during its separation is a common complication which is encountered in 15% of cases.
One should be careful at the time of dissection and if there is spillage of stone each stone should be removed from the peritoneal cavity to avoid abscess formation in future.
Extraction of Gallbladder

The gallbladder is extracted through the 11 mm epigastric operating port with the help of gallbladder extractor. Many surgeons use umbilical port for withdrawal of gallbladder. First the neck of the gallbladder should be engaged in the cnula and then canula will withdraw together with neck of gallbladder held within the jaw of gallbladder extractor. Once the port with the neck of the gallbladder is out the neck is grasped with the help of a blunt hemostat and it shoud be tried to pull out with screwing movement. If gallbladder is of small size it will come without much difficulty otherwise small incision should be given over the neck of the gallbladder and suction irrigation instrument should be used to suck all the bile to facilitate easy withdrawal.
Some time big stones will not allow easy passage of gallbladder and in these situation ovum forceps should be inserted inside the lumen of gallbladder through the incision of its neck and all the stone should be crushed.

The Instrument and then ports are removed. Telescopic should be removed leaving gas valve of umbilical port open to let out all the gas. At the time of removing umbilical port telescope should be again inserted and umbilical port should be removed over the telescope to prevent any entrapment of omentum. The wound should be closed with Suture. Vicryl should be used for rectus and Un-absorbable intra-dermal or Stapler for skin. Some surgeon likes to inject local anaesthetic agent over port site to avoid post operative pain. Sterile dressing over the wound should be applied.
Complications:
Early complication:
- Common bile duct injury
- Bile leak
- Injury to viscera
- Hemorrhage
- Retained stones and abscess formation
Late complication:
- Biliary strictures
- Cystic duct clip stones
- Hemorrhage
Lap Chole and CBD injury
Please!
"Revert to open if unsure about Anatomy"
Incidence of Iatrogenic CBD injury is 0.12% and 0.55% during open and laparoscopic cholecystectomy respectively
Common cause of CBD injury:
- Misinterpretation of anatomy 70%
- Technical Errors
- Risk factors
- Surgeon operates on image rather than reality
- Visual psychological studies has shown that laparoscopic surgeon works on snap interpretation by brain and success or disaster depends on whether snaps are right or wrong
Snap interpretation will be wrong if there is:
- Eye ball degradation
- Lack of Initial identification and memory of key structure to the point of absolute certainty.
- Most important technical error is hilar bleeding and frantic attempts are made to control bleeding by electrosurgery.
In case of bleeding
- First apply pressure
- Take suction irrigation and atraumatic grasper
- Apply electrocautery only when bleeding point is identified
Type of CBD Injury
BISMUTH CLASSIFICATION
- Type 1 - CHD stump > 2 cm.
- Type 2 - CHD stump < 2 cm.
- Type 3 - Hilar, Rt. and Lt. duct confluence intact
- Type 4 - Hilar, separation of Rt. and Lt. ducts
- Type 5 - Injury to aberrant Rt. duct � CBD injury
If complication recognized intra operatively:
- For high complete transaction Roux-en-Y hepaticojejunostomy
- For lower complete injuries primary suture repair over T tube
- Long end of T tube must not be exteriorized from same site
- For partial injuries Insertion of T tube and Roux-en-Y serosal patch
Strategy to handle complication recognised post operatively:
- USG + ERCP + MRCP
- Fluid + Electrolyte + systemic antibiotic
- Conservative treatment and biliary drainage for 6 weeks by ERCP stent insertion or
- PTBD (Percutaneous trans hepatic biliary drainage) if Endoscopic stent application is not possible
- After Several weeks Reconstructive surgery
- Roux-en-Y Choledocoduodenostomy or Hepatojejunostomy
How to avoid injury?
- Try to memorise initial anatomy of Calot's triangle
- A large distended Gall bladder should be aspirated and lifted rather than grasped
- Antero-lateral traction is better than fundus pull to avoid tenting of CBD
- Avoid meticulous dissection by energized instrument
- Better to do skeletanization through pledget
- During detachment of gallbladder from liver bed maintain plane of adipose tissue
- Use Suction Irrigation frequently
Tenting of the CBD should always kept in mind at the time of dissection to avoid injury.





