Laparoscopic Port Closure Technique
Minimally, invasive laparoscopic surgery has revolutionized the way surgery is performed for an increasing number of patients. Incisional hernia can occur after any abdominal surgery and laparoscopic surgery is not immune to this complication. The hernia that follows laparoscopy usually occurs through the larger ports (size greater than 10 mm), especially the umbilicus.
Predisposing factors include:
• Previous laparoscopies
• Extensive manipulation during surgery
• Increased intra-abdominal pressure
• Obesity
• Use of sharp cutting-tip trocars
• Rapid abdominal deflation at the end of surgery
• Poor port removal techniques and defective closure of the abdominal fascia
• Wound extension
• Male sex
• Infection of the wound
• Pre-existing umbilical defects
• Postoperative chest infections
• Pre-existing diseases such as diabetes mellitus
• Connective tissue disorders
• Job profile of the patient (weight lifting).
Among all these factors, the single most important factor remains the improper closure of the fascial defects at the port sites. The diagnosis is often delayed because most cases present late, and treatment might be instituted along other lines. Computed tomography scans are helpful in its diagnosis and will facilitate prompt treatment to avoid the grave consequence of bowel gangrene. The hernia may become evident at any time following laparoscopic surgery and the patient may either have an uncomplicated hernia or may be afflicted with a variety of complications such as evisceration of the bowel or omentum and it may become a cause of significant morbidity. Meticulous closure of the fascia, avoidance of unnecessary wound extension, the use of non-absorbable sutures when faced with defects more than 2 cm in size, completely defining the extent of any pre-existing hernia and repairing this at the time of port site closure, are recommended to minimize the incidence of port-site hernia after laparoscopic surgery.

Proper closure of port greater than 10 mm is essential to prevent hernia
Whilst surgical techniques and instrumentation have made significant advances, it is usual that the surgical incision is closed using invasive suturing techniques or by the use of tapes or by the use of topical cyanoacrylate skin adhesives (TCAs) for the closure of surgical wounds. The incidence of incisional hernia occurring at the port sites after laparoscopic surgery lies between 0.02 to 3.6 percent and usually remains unreported, until the development of complications.

Incisional hernia development due to improper closure of port should be repaired later by mesh
Any port closure technique should have the following characteristics:
• Effective (strong and secure) surgical wound closure
• Faster wound closure
• Better scar cosmesis
• Occlusive microbial wound dressing
• Less tissue trauma, reduced inflammatory reaction
• No requirement for suture/staple removal
• Easy to use/simple learning curve
• Reduced risk of needlestick injury—safety and costs
• Cost-effective.
Withdrawl of Instruments and Ports
Once the surgery is finished, all the instruments should be removed carefully under vision. All the accessory port should be removed and the gas is removed by releasing the valve of 10 mm cannulas. The primary port should be taken out in the end. If the last port is suddenly withdrawn, the sudden suction effect of the cannula can pull the omentum or bowel inside the port wound, the chances of port site hernia and adhesion are much higher in this case. It is a good practice to insert some blunt instrument or telescope inside the abdomen while removing the last cannula out over that instrument, to prevent inadvertent entrapment of omentum or bowel. The access technique will result in a breach in the continuity of the abdominal wall which needs to be repaired at the end of surgery. All the 10 mm or greater than 10 mm port should be repaired properly to prevent any future possibility of a hernia. The rectus sheath should be sutured with vicryl. Only one stitch is required in the middle which will convert 10 mm wound into 5 mm. The 5 mm port wounds are not necessary to repair.

The tip of the telescope should be introduced in and the cannula is pulled over the telescope to prevent suction of omentum or bowel
Laparoscopic Port Closure Instruments
Various types of port closure instruments are available. The suture passer is a convenient instrument for port closure. It is used to pass the thread on the side of the cannula and then it is tied externally.
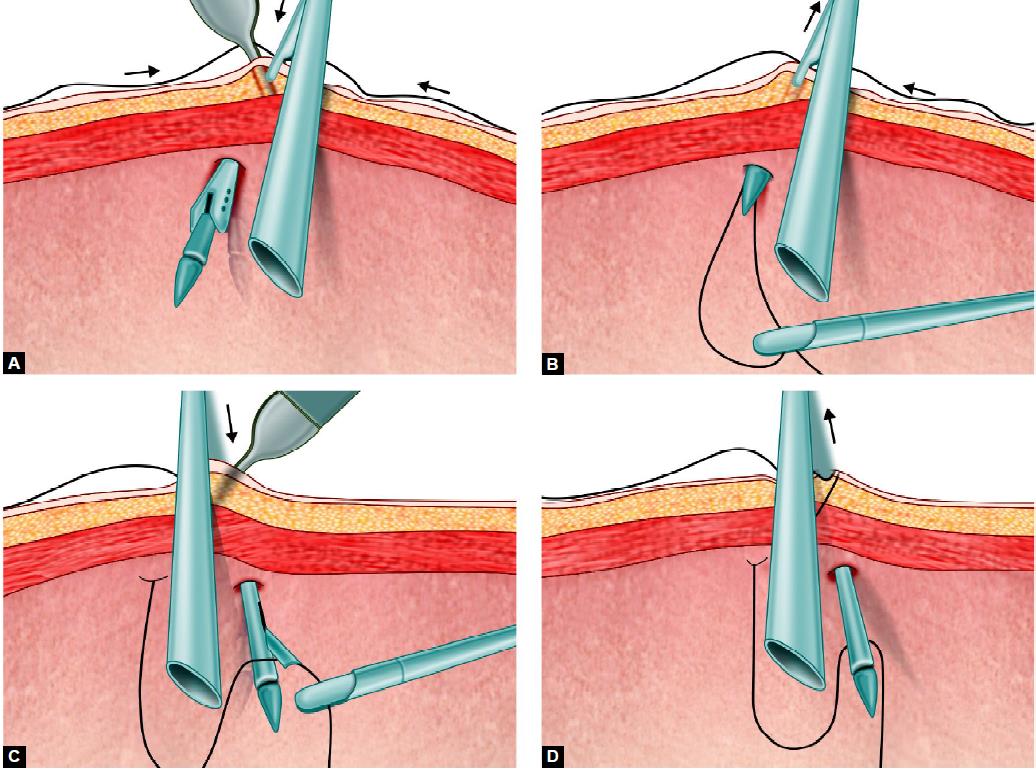
Port closure with the help of suture passer
Port Closure Needle
This is a simple instrument just like cobblers and it can be effectively used for closing the port. The tip of the instrument is blunt and the needle faces towards the fascia, so the chances of injury to the bowel are less with the use of this instrument. Aneurysm needle can also be used for closing fascia. The advantage of this needle is that eye is at the tip and due to rigid structure, there is no risk of bending or rotation of the needle. After closing the rectus sheath the skin can be closed by intradermal, skin stapler or any of the surgical skin glues topical cyanoacrylate skin adhesives (TCAs) available.

Port closure needle

Aneurysm needle

Closure of skin wound by skin stapler.





