
ROLE OF O.T. TABLE HEIGHT ON THE TASK PERFORMANCE OF MINIMAL ACCESS SURGERY.
Dr. Gurvinder Kaur; Prof. Dr. R. K. Mishra
Project Submitted Towards Completion Of Diploma In Minimal Access Surgery, World Laparoscopy Hospital, Gurugram, NCR Delhi, India. April 2007.
Abstract:
The advent of laparoscopic surgery has changed the concept of surgery from prolonged painful to painless, cosmetically satisfying and short stay. In the past few years many instruments have been developed and introduced into the operating room (OR), but there has been ongoing debate about the optical ergonomic posture of the operating surgeon.
One of the main ergonomic problem in our currently available operating room table is that they are they are designed for the open surgery and are not ideal (suitable) for the laparoscopic surgery. Since laparoscopic surgery requires the use of longer instruments than open surgery thus changing the relation between the height of the surgeon and the desirable height of the operating room table.
This study aims to understand an ergonomically optimal operating table height required for the particular height of the surgeon from the floor so that they can perform their surgery comfortably.
The operating table height was defined as the upper level of the table from the floor. The study was undertaken keeping all other variables fixed (Elevation angle, Manipulation angle, Azimuth angle, Distance of monitor.) Co-axial alignments were maintained. The only variable was the operating room (OR) table height.
Keyword:
Ergonomics, Laparoscopy, Operation Table Height.
Definitions:
Elevation Angle: It is an angle between the instrument and the body of the patient.
Manipulation Angle: It is an angle between the two working instruments.
Azimuth Angle: It is an angle between the one side of instrument and the telescope.
Co-axial Alignment: The axis joining the eye of the surgeon, target of dissection and the center of monitor.
Introduction:
Ergonomics is the study (or science) of the interaction between human and their working environment in terms of equipment design, work place layout the working environment, safety, productivity and training. Often called the "human factors" in the United States, it is the psychological and physical interaction between the user (e.g. surgeon, assistants or nurse ) and their tools.(1)
Since the past fifteen years laparoscopic surgery has become part of the visceral surgery, providing the patient short painless and a quick recovery. In the literature laparoscopic surgery is in many cases associated with ergonomics problems (2-4). Infact poor ergonomics has always been one of the major drawbacks of endoscopic surgery.In the last decade or so, many new instruments and devices have been developed for the laparoscopic surgery. The handling of these tools has a sizeable impact on the length of the procedure in terms of time and the overall morbidity. The relationship between the surgeon and the tools also determine how much effort is expended by the surgeon.
The fatigue and discomfort of the surgeon's complaints during laparoscopy have led to several studies which investigate the origin of the physical problems (5-9).
A comparative study of the surgeon's posture during open and laparoscopic surgery (6) showed more upright head and back posture with less body movements during laparoscopic surgery. There were significant musculoskeletal complaints of neck and arms. One study has shown that laparoscopy instruments causes excessive flexion and ulnar deviation of the surgeon's wrist with abduction of arm during manipulation (7-10). This ergonomic problem results from the combined effect of the fixed point of insertion of the laparoscope through the body wall, a large external arc of the arm movement due to greater length of the instrument and the poorly adjusted operating table height.
The Society Of American Gastro-intestinal Endoscopic Surgeons (SAGES) realized the importance and established a study group for improving the ergonomics in the operating room.(11-13). De Quervain pointed out the importance of adjusting of the table for the positioning of the patients in relation to the surgeon for open surgery (14-15). In laparoscopic surgery the situation differs, since the table cannot be lowered sufficiently for precise and relaxed work. To overcome this problem the surgeon compensates by elevating their arms which is fatiguing (16).
Guidelines for the height of the work surfaces for standing workers in industry or offices have existed for many years (17). In medical literature, there has been, however, less focus on the ergonomics problem of operating table height during laparoscopy. Only recently a paper has been published dealing with the ergonomic problem of incorrect operating table height (18).
This aim of the study was to find out the ergonomically optimal operating table height required for the particular height of the surgeon for laparoscopic surgery in order the surgeon can perform their task comfortably without the extreme upper limb joint movements. The approach of this study can be extended as guidelines for designing of the ergonomically optimal operating table.
Material and Method:
The study was carried out in the Laparoscopic Laboratory of World Laparoscopy Hospital, Gurugram, NCR Delhi. A literature search was also performed using Medline and the search engine Google to find out for any such related article. The following search terms were used "ergonomics" "ergonomics in surgery", "ergonomics in laparoscopy".
The tests were performed on endo trainer using the six different table heights for a particular surgeon for task performance. All the other variables were kept fixed or constant (Elevation angle, Manipulation angle, Azimuth angle, Distance of the Monitor). The co-axial alignments were maintained. The only variable studied was the OR Table Height.
The ports were introduced keeping in mind the "base-ball diamond" concept (19).
1) The telescope was fixed in between the working instruments.
2) Level 1 lever system was used for the insertion of the instrument through the ports i.e. half the instrument was inside and half the instrument was kept outside maintaining the Elevation angle of 30 degree.
3) Manipulation angle was fixed to 60 degree.
4) Azimuth angle was fixed to 30 degree.
| Joint | Movement | Neutral Zone (degree) |
|---|---|---|
| Shoulder | Abduction | <30 |
| Elbow | Flexion Extension | >30 <130 0 |
| Wrist | Ulnar abduction Radial abduction Palmer Flexion Dorsal flexion | <15 <15 <15 <15 |
Table 1- Neutral zone of joint movement (VAN VEELEN)
The joint movement and the angles (abduction of the shoulder and flexion of the wrist) of the shoulder elbow and wrist were measured by video recording and snap shots during the task performance.
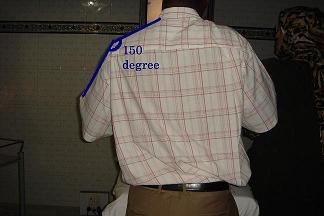
Fig 1. Abduction of the shoulder were measured.

Fig 2. Flexion of the wrist and elbow were measured
The results were evaluated by a questionnaire and snap shots. The optimum operating table height was defined for the different height of surgeon. The girth of the patient was kept constant during the study as the task was performed on the endo-trainer

Fig 3: Operating table height
Task: The subject had to perform the task of tying the intracorporeal knot. The operating table height was adjusted to six different height for a particular surgeon. The monitor was placed in front of the surgeon at a height of 170 cm from floor.
Subjects: Consisted of surgeon and laparoscopic trainees. The total numbers of subjects were twenty five out of which five were females and the rest twenty were. They worked mostly with right hand.
Operation Table Height: Six different heights of the operating table was adjusted varying from 65 cm to 90 cm.
Duration of Each Observation: The duration of each observation was for five minutes for each height of operating room table. For six different heights of the table the total observation duration was of 30 minutes for the task performance with respect to the position of shoulder, elbow and wrist movements.
Video analysis: The camera was used to record the position of the shoulder, hand arm and wrist joint and videos snaps were taken during the task performance at different operating table height.
Questionnaire: The subjects were asked for the particular level of discomfort of the operating table height during their task performance.
Level of comfort (from best to worst) was graded:
A-Comfortable: when the subject's upper extremities were in neutral zoneposture.
B-Less Comfort: when there was minimum deviation from the aboveposture (Abduction of shoulder joint and flexion of wrist joint).
C-Discomfort: When there was increasing abduction of shoulder joints with increasing flexion of wrist joint to perform the task.
D-Uncomfort : When there was complementary increased abduction of shoulder joint with increased flexion of wrist joint to perform the task.
Results:
The results of the level of comfort of OR table during task performance with respect of the height of the surgeon is shown in Table 1.The short stature subjects (147 cm -151 cm) were comfortable at 65 cm table height while the tall subjects (178-182 cm) experienced comfort at 90 cm OR table height.
The maximum subjects were in the height group 165-170cm which is the average height of the Indian masses, were comfortable during their task performance at 80 cm OR table height.
There was a parallel steady rise in trend (Graph 1). As the height of the surgeon increased there was proportionate increase in the vertical height of the OR table.
The results of the video analysis are shown (Table 2). For 155cm subject height was comfortable at 70 cm in the neutral zone posture showing shoulder joint was abducted at 15 degree and elbow joint showed extension at 125 degree abduction of wrist joint.
At 65 cm OR table height there was less comfort experienced by the subject as the shoulder joint was abducted to zero degree and the elbow joint extended to more than 130 degree (i.e 150 degree). On further raising the table height to 75 cm there was the same less comfort. The shoulder joint was abducted to 40 degree with extension of the elbow joint to 120 degree to perform the task.
When the OR table height was further raised to 85 cm there was discomfort experienced by the subject since the abduction of shoulder joint had increased further to 45 degree combined with the increasing flexion of wrist joint to perform the task. At 90 cm for the particular surgeon height there was uncomfort felt by surgeon during task performance. This was compensated by the complementary increased abduction of shoulder joint (75 degree) and then elbow joint was straightened, also there was increased flexion and ulnar deviation of wrist joint.
The different grades of comfort level as stated by the surgeon during the task performance at the six different OR table height is shown in (Table 3). The result of the objective evaluation with video analysis co-relate with the subjective assessment of the comfort level of the subjects (questionnaire) working at the particular vertical height of the OR table.
The height of the operating table varies in relation to the surgeon's level of comfort for task performance.
| Subject (Surgeon Height cm) | Comfort of the level of OR Table height (cm) |
|---|---|
| 147 | 65 |
| 150 | 65 |
| 151 | 65 |
| 155 | 70 |
| 156 | 70 |
| 160 | 75 |
| 160 | 75 |
| 161 | 75 |
| 163 | 75 |
| 164 | 75 |
| 165 | 80 |
| 165 | 80 |
| 166 | 80 |
| 167 | 80 |
| 167 | 80 |
| 168 | 80 |
| 168 | 80 |
| 170 | 80 |
| 171 | 85 |
| 172 | 85 |
| 173 | 85 |
| 174 | 85 |
| 178 | 90 |
| 180 | 90 |
| 182 | 90 |
Table 1: Subjects Height versus Table Height (Comfort level)
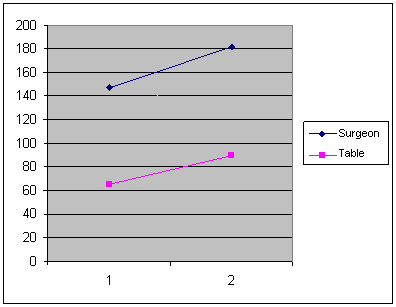
Graph 1: Relation between Surgeon and OR Table Height(cm)
| O.T. Table Height(cm) | Abduction Angle of Shoulder | Flexion of Elbow and wrist | Observation |
|---|---|---|---|
| 65 |  0 degree 0 degree |  150 Degree 150 Degree | B= Less Comfort Minimal deviation from neutral zone posture. |
| 70 |  15 Degree 15 Degree |  125 Degree 125 Degree | A= Comfortable- neutral zone posture shoulder joint abducted 150 elbow extended 1250 wrist joint extended. |
| 75 |  40 Degree 40 Degree |  120 Degree 120 Degree | B= Less Comfort Minimal deviation from neutral zone posture. |
| 80 |  45 Degree 45 Degree |  115 Degree 115 Degree | C= Discomfort starting of abduction of shoulder joint, increasing flexion of elbow joint, flexion & ulnar deviation of wrist joint |
| 85 |  60 Degree 60 Degree |  105 Degree 105 Degree | C= Discomfort starting of abduction of shoulder joint, increasing flexion of elbow joint, flexion & ulnar deviation of wrist joint |
| 90 |  75 Degree 75 Degree |  Angle can not be calculated from side(awkward position) Angle can not be calculated from side(awkward position) | D= Uncomfort complementary increased abduction of shoulder joint 750 increased flexion & ulnar deviation of wrist joint |
Table 2: Subjects Height versus Table Height
| Height of subject (cm) | O.R Table Height(cm) and Grade of Comfort Level | |||||
|---|---|---|---|---|---|---|
| 65 | 70 | 75 | 80 | 85 | 90 | |
| 147 | A | B | B | C | D | D |
| 150 | A | B | B | B | C | D |
| 151 | A | B | B | C | C | D |
| 155 | B | A | B | C | C | D |
| 156 | B | A | B | B | C | D |
| 160 | B | B | A | B | C | D |
| 160 | B | B | A | B | C | D |
| 161 | C | B | A | B | C | D |
| 163 | C | B | A | B | C | D |
| 164 | C | B | A | B | C | D |
| 165 | C | C | B | A | B | C |
| 165 | C | C | B | A | B | C |
| 166 | C | C | B | A | B | C |
| 167 | C | B | B | A | B | C |
| 167 | C | C | B | A | B | C |
| 168 | C | C | B | A | B | C |
| 168 | C | C | B | A | B | C |
| 170 | B | B | B | A | B | C |
| 171 | C | C | B | B | A | B |
| 172 | C | C | B | B | A | B |
| 173 | C | C | B | B | A | B |
| 174 | C | C | B | B | A | B |
| 178 | D | C | C | B | B | A |
| 180 | D | C | C | B | B | A |





