Frequently asked question about LAVH
(Laparoscopic assisted vaginal hysterectomy)

Click here to see full video of LAVH Abdominal + Vaginal Part. (32 MB)
What is LAVH ?
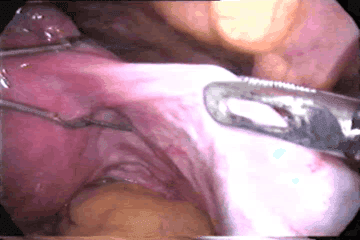
LAVH is increasingly becoming popular. Nowadays it is definite alternative to abdominal hysterectomy. It is removal of un prolapsed uterus with the help of laparoscopy. Many women come to the doctor and say they want a "laser" hysterectomy. What they usually mean is a LAVH. The technique used to use lasers but now lasers have been mostly replaced by surgical clips, cautery or suturing. First lap hysterectomy was done by Reich et al in 1989. It's really a technique made to replace abdominal hysterectomy.
What are the Indications of LAVH ?
Indications are:
- Previous pelvic surgery
- Endometriosis
- Previous C.S.
- Pelvic pain
- Suspected adnexal pathology
- Uterine myoma
- Ectopic pregnancy
- Acute or chronic pelvic inflammatory disease
- Minimum uterine mobility & limited access
If a hysterectomy can be performed in the first place, there would be no point in adding the costs and complications of laparoscopy. Its greatest benefit is the potential to convert what would have been an abdominal hysterectomy. An abdominal hysterectomy requires both a four to six inch long incision in the abdomen, which is associated with greater post-operative discomfort and a longer recovery period. Another advantage of the LAVH may be the removal of the tubes and ovaries which on occasion may not be easily removed.
The most common medical reasons for performing hysterectomies include uterine fibroids (30 percent of cases), abnormal uterine bleeding (20 percent), endometriosis (20 percent), genital prolapse (15 percent), and chronic pelvic pain (about 10 percent). For most of these conditions, other treatments should first be considered, and hysterectomy should be reserved as a last resort.
What are the benefits of LAVH ?
LAVH result in a significantly shorter hospital stay, with a much more rapid return to normal activities, than TAH (Total Abdominal Hysterectomy). The drug requirement to control pain and the level of pain, patients experienced were also significantly less. Blood loss is not different for the two procedures.
Postoperative recovery times and pain levels were assessed in 37 patients with a primary complaint of pelvic pain and diagnoses of fibroid uterus, adenomyosis, and severe endometriosis who underwent LAVH. Women reported an activity level of 8.7 on a scale of 1 to 10 (10 no limits on activity) by postoperative day 14. In another study those undergoing abdominal hysterectomy had a mean uterine weight of 418 g compared with 150 g for those undergoing LAVH. The hospital stay after abdominal hysterectomy was 4.5 days and after LAVH 2.5 days. An important public policy issue now confronts us. As it is currently performed, LAVH is more expensive than TAH (Total Abdominal Hysterectomy). The issue is whether the benefits of shorter convalescence and faster return to the work force, shorter hospitalization, and less need for narcotics for postoperative pain outweigh the disadvantage of the higher cost. If total health care system costs are evaluated, the short-term disability costs of 2 weeks of recovery after laparoscopic hysterectomy should be compared with disability costs of 6 to 8 weeks of recovery after abdominal hysterectomy. The woman who returns to work 4 to 6 weeks earlier is producing. For LAVH to be economically viable compared with TAH, savings in disability costs and the increased contribution to the gross domestic product must offset the increased health care costs.
In the current system, insurance companies and hospitals do not share in these benefits, only the costs. The economic impact of laparoscopic surgery must take into account both the cost to the hospital and insurance payers and these productivity and social issues. Insurance is based on a risk pool whereby the cost of a premium is based on the cost of treatment, not the ability of the subscriber to return to work. An economic and social cost-benefit analysis must be performed before decisions are made to modify or judge a procedure that provides substantial benefits to the patient. Since its introduction in 1989, continued improvement of techniques will likely progress rapidly so that LAVH will be performed on an outpatient basis for many women, and will result in shorter recovery time.13 thus the increased operating room time of approximately 46 minutes is significantly outweighed by the benefits available with widespread application of this procedure.
What are the types of LAVH ?
Garry and Reich classification:
- Type 1 - diagnostic lap + VH
- Type 2 - lap vault suspension after VH
- Type 3 - LAVH
- Type 4 - LH (lap ligation of uterine art.)
- Type 5 - TLH
- Type 6 - LSH (lap supra-cervical hysterectomy)
- Type 7 - LHL (lap hysterectomy with lymhadenectomy)
- Type 8 - LHL + O (as above + omentectomy)
- Type 9 - RLH (radical lap hysterectomy)
What are the Preoperative measures necessary before LAVH ?
- Catheterization
- Bowel preparation
- Routine Anaesthetic and Medical checkups
- Peglac powder - 1 sachet with water a night prior
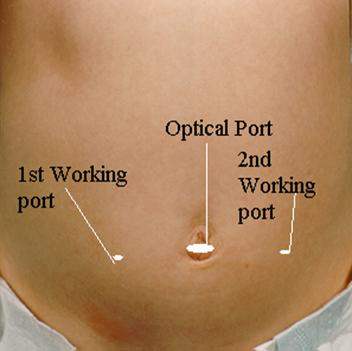
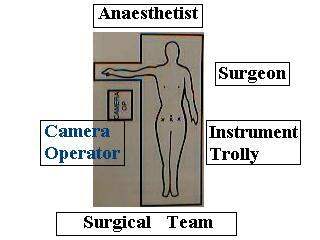
What are the port position, patient position and position of surgical team at the time of LAVH ?
- Steep trendelenberg position for laparoscopic part
- Lithotomy position
What is the benefit of of LAVH ?
Laparoscopic management provide less postoperative morbidity. Laparoscopic management is a useful method for reducing hospital stay, complications and return to normal activity.The main advantages are:
- Less post-operative pain
- Faster recovery
- Short hospital stay
- Less post-operative complications like wound infection and adhesion
- Cost-effective in working group
Is every patient fit for LAVH ?
No. Most surgeons would not recommend laparoscopic treatment in those with previous chronic diseases.
Patients with cardiac diseases and COPD should not be considered a good candidate for laparoscopic management. LAVH may also be more difficult in patients who have had previous lower abdominal surgery. The elderly may also be at increased risk for complications with general anaesthesia combined with pneumoperitoneum. Laparoscopy does add to the surgical risk in patients with a lowered cardio-pulmonary reserve with regard to the consequences of the pneumoperitoneum and a longer operative time.
What are the complications of LAVH ?
In experienced hand there is not any specific complication directly related to laparoscopic procedure but if the surgeon is not trained enough in laparoscopy than the chance of following complication is there:
Missed diagnosis
Bleeding
Incomplete removal of
Visceral Injury
Leakage of purulent exudates
Intra-abdominal abscess
Hernia
But inexperience hand these complications are extremely rare. and altogether laparoscopic procedure has less complication than conventional surgery
Minimal Access Surgeon





