The word nephrectomy means elimination of a kidney. A kidney can be removed either utilizing an ‘open’ surgical approach or using ‘keyhole’ (laparoscopic) surgery. Open surgery to get rid of a kidney involves making a large cut on the side with unavoidable problems for example pain, a hospital stay of 7-10 days, and a prolonged time off work work. The more modern laparoscopic approach to kidney removal uses 3 or 4 one centimetre cuts (incisions). A thin tube with a light and camera on the end (a laparoscope), and surgical instruments may then be passed through these incisions. The camera sends pictures to a TV screen so that the surgeon can easily see the kidney and surrounding tissue. One from the incisions is going to be enlarged make it possible for the kidney to pass through once it has been disconnected in the surrounding tissues and blood vessels.
A laparoscopic nephrectomy is performed under a general anaesthetic. You will meet the Anaesthetist on the day of the operation and that he or she'll discuss the anaesthetic with you. You should expect to stay in hospital for 2-4 nights. The laparoscopic method of kidney removal has been shown to cause less loss of blood and fewer complications compared to open method, as well as includes a shorter recovery time. The open surgical method of kidney removal has become only employed for complicated cases.
So why do I need a nephrectomy?
A kidney should be removed for a number of reasons. These are outlined below:
- The kidney may be only partially working, or not working at all. If left in place it's really a source of repeated infections and pain.
- Infection may have damaged the kidney so that it requires removal.
- A cancer arising inside the kidney was diagnosed. The usual treatment for this is to take away the affected kidney.
- If a cancer has been discovered in the kidney, it's occasionally essential to remove the adrenal gland, which lies on top of the kidney, at the same time.
- For some kidney cancers, there's a high risk of cancer recurrence in the ureter (the tube which carries urine from the kidney to the bladder). If this kind of cancer has been discovered, you will need a little incision low recorded on your abdominal wall, as well as the kidney operation described.
The reason behind removing your kidney will be discussed along with you. Before the operation is completed it is usual to perform various scans and blood tests so that the surgeon has just as much details about the diseased or cancerous kidney as you possibly can. These tests also make sure that the remaining kidney is working normally. Providing how the remaining kidney is functioning normally you will not desire to make any change to your lifestyle (eg diet) or activities following the operation. Possible results in the procedure are outlined below. However, for those who have any concerns please discuss all of them with nursing and medical staff because it is essential that you understand what will occur to you. You is going to be asked to sign a consent form before undergoing the operation but you may withdraw your consent at any time. Some patients experience temporary shoulder tip pain and abdominal bloating every day and night following the operation. This are closely related to inflation of the abdominal cavity with gas throughout the operation. Using the retro-peritoneal approach decreases this side effect. Mild painkillers are often adequate to control the pain. Occasionally following this operation, infection, or a hernia, may exist in a number of from the incisions requiring further treatment. This happens very rarely when the surgeon uses the retro-peritoneal approach.
Rare Complication
- Bleeding can occur throughout the surgery such that the surgeon needs to abandon the keyhole approach and employ the conventional open approach to kidney removal. If this happens a blood transfusion may be required.
- During the operation the lung cavity might be entered which is repaired during the procedure without any extra incisions.
Unusual
- Recognised (and unrecognised) injury to surrounding organs or arteries may occur, requiring conversion towards the open surgical approach, or deferred open surgery.
- Problems with the anaesthetic, or heart or circulation system complications may occur requiring admission towards the Intensive Care Unit. Such complications incorporate a chest infection, clot/s on the lungs or perhaps in the legs, a stroke or perhaps a cardiac arrest. These are not specific to laparoscopic procedures.
What happens prior to the operation?
You will usually attend a pre-assessment clinic before your operation. The purpose of this appointment would be to organise anymore tests which may be needed, and check your fitness for that operation. A member of the nursing staff and one from the doctors in the surgeons team will see you.
It is useful should you bring in a list of any medicines that you simply normally take at home, and let us know associated with a drug allergies you might have.
It is necessary how the hospital know if you are on any drugs that thin the blood e.g. Aspirin, Warfarin, Clopidogrel, Dipyridamole.
If you're taking Warfarin it may be essential to bring you into hospital a couple of days before your operation, or to change your Warfarin to an injection that may be given in your own home.
Several obstacles are preventing Laparoscopic Nephrectomy technique from being more widely embraced. The first is the time factor which is considerably longer than for an open nephrectomy. The second is the handling of the renal pedicle. Clayman and coworkers have used titanium clips to secure the renal artery and vein. Ehrlich and coworkers used an endoscopic linear stapler to secure the pedicle. Despite the fact that Clayman and coworker's group did not report any significant intraoperative or postoperative bleeding because of inadequate pedicle control, many urologists are uneasy with this aspect of the operation. The third and perhaps most seri–ous concern is the applicability of this technique to cases of renal malignancy. Currently, the adrenal gland is not included in the laparoscopic radical nephrectomy; although this exclusion is probably more a theoretical concern in lower pole and midpole tumors, it would be a limiting factor in upper pole tumors.
Tumor spillage during any laparoscopic procedure is an obvious practical concern. Several reports documented tumor implantation during laparoscopy. Clayman and coworkers tried to solve this problem by developing an entrapment system for the kidney and the lymph nodes. These systems con–sist of impermeable bags inserted through the laparoscopic tro–car. The surgical specimen is placed within the bag or pouch and a drawstring around the opening of the bag allows for clo–sure and acts as a handle to remove the pouch from the abdom–inal cavity through the laparoscopic trocar. In nephrectomy, the renal specimen is fragmented and aspirated using a specially designed electrical tissue morcellator placed through the neck of the kidney sack. The development of this type of technology decreases but does not eliminate the potential for tumor spillage. Undoubtedly, more work is needed to address the con–cern of tumor implantation, if this technique is to be applied to malignant renal tumors.
Operative Technique
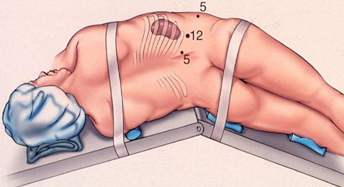
After induction of general anesthesia, a occlusion bal–loon catheter is passed up the ureter of the kidney to be removed. A bladder drainage catheter is also used as well as a nasogastric tube. The patient is placed in a supine position. A Veress needle is placed at the umbilicus, and a carbon dioxide pneumoperi–toneum is created in the usual manner. Then two 11mm laparoscopy ports are placed, one at the umbilicus and one imme–diately subcostal along the midclavicular line. A 5mm port is also placed in the midclavicular line, 2 to 3 cm below the level of the umbilicus. The patient is then placed in the lateral decubitus posi–tion and secured to the operating table. Two 5-mm ports are placed in the anterior axillary line, one on a level with the umbili–cus and one off the tip of the eleventh or twelfth rib.
Dissection commences by incising the line of Toldt and resecting the colon medially. The ureter is then identified and secured with a 5-mm locking forceps. The lower pole lateral sur–faces, upper pole lateral surfaces, and upper pole of the kidney are dissected free. The adrenal gland is left in place. The kidney is then lifted upward, which places the renal hilum on traction. The renal artery and vein are then dissected. Three endosurgical clips are placed on the distal portion of each vessel, and two clips are placed on the proximal portion of each vessel; an endoscopic scissors is then used to divide the vessels.
The ureter is divided between two clips and the kidney is free. An impermeable nylon surgical sack is introduced through an 11-mm port. Three 5–mm graspers are used to open the mouth of the sack, and the kidney is pushed into the open sack. The drawstrings on the sack are grasped by a 5-mm forceps and pulled through the 11–mm umbilical port, thereby closing the neck of the sack on the kidney. The mouth of the sack is then brought out through the skin, and the metal shaft of the electrical tissue morcellator is introduced into the sack. The morcellator is activated, and the renal tissue is fragmented and aspirated. When all the renal tissue is removed, the empty sack is removed from the abdomen. The port sites are closed in the standard fashion.
In the two cases of transitional cell carcinoma , the ureter was dissected down to the bladder, and a laparoscopic GIA sta–pler was used to include the distal ureter and a cuff of bladder. Clayman and coworkers and Gaur and coworkers also described a retroperitoneal approach to laparoscopic nephrectomy. A key advance to this approach has been the use of a retroperitoneal balloon dissector that facilitates the development of working space within the retroperitoneal space.




