Introduction:
Gastrostomy is palliative surgical procedure for inserting a feeding tube through the abdomen wall and into the stomach. Gastrostomy is generally performed in a patient who are temporarily or permanently needs to be fed directly through a tube in the stomach. Now a days the best option for these patient is first to try percutaneous endoscopic gastrostomy.
The technique of percutaneous endoscopic gastrostomy is the "pull" method introduced by Gauderer and Ponsky in 1980. Many modifications of the original pull technique has been done. Now a days the gastrostomy tube can be pushed rather than pulled into place by a "push" method. In another modification, the "introducer method," the stomach is directly punctured and a feeding tube placed over a guide wire. Percutaneous gastrostomy has also been described without endoscopy using a nasogastric tube or gastric insufflation, fluoroscopic monitoring, and a direct percutaneous catheter insertion technique. The basic elements common to all of these techniques are:
- Insufflation of stomach to bring into apposition to the abdominal wall.
- Percutaneous placement of a tapered cannula into the stomach.
- Passage of a suture or guide wire into the stomach.
- Placement of the gastrostomy tube.
Patient selection:
Laparoscopic gastrostomy is indicated when a percutaneous endoscopic gastrostomy (PEG) cannot be performed or is contraindicated. Specific situations in which this is likely to occur include:
- An obstructing oro-pharyngeal lesion.
- A lesion in the esophagus and reconstruction is not possible.
- Some time colon or omentum are overlying the stomach so percutaneous blind approach is not possible in these patients laparoscopic Gastrostomy is the best option.
Methods:
Two methods of laparoscopic gastrostomy has been described. The first method constructs a simple gastrostomy without a mucosa-lined tube. This method is appropriate for most indications. The tract will generally seal without surgical closure once the tube is removed.
An second method utilizes the endoscopic stapler to construct a mucosa-lined tube in a fashion analogous to the open gastrostomy. This provides a permanent stoma which can be easily re-cannulated.
It appears that the laparoscopic approach has several advantages:
- Cosmetically better outcome.
- Less tissue dissection and disruption of tissue planes
- Less pain postoperatively.
- Low intra-operatively and postoperative complications.
- Early return to work.
The main tasks of this operation consist of:
- Preparation of the patient.
- Creation of pneumoperitoneum. Insertion of port.
- Diagnostic laparoscopy
- Exposing the Anterior Wall of the Stomach and Identifying the Site of tube Insertion
- Insertion of Gastrostomy tube in the abdominal Cavity
- Insertion of Gastrostomy Tube in the Stomach
- Securing the Gastrostomy
- Irrigation and suction of operating field.
- Final Diagnostic laparoscopy for any bowel Injury or haemorrhage.
- Removal of the instrument with complete exit of CO2. Closure of wound.
Operating technique:
Patient Position
- The patient is placed on the operating table in supine position.
- The operating table is tilted head up by approximately 15 degree.
- Compression bandage are used on leg during the operation to prevent thromboembolism.
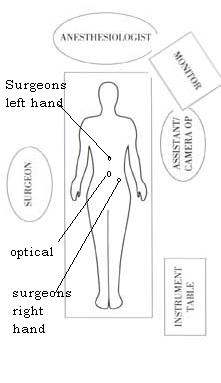
- The surgeon stands between the patient's right side.
- The first assistant, whose main task is to position the video camera, sits on the patient's left side.
- The instrument trolley is placed on the patient's left allowing the scrub nurse to assist with placing the appropriate instruments in the operating ports.
- Television monitors are positioned on either side of the top end of the operating table at a suitable height so surgeon, anaesthetist, as well as assistant can see the procedure.
Anaesthesia: General Endotracheal Anaesthesia is used. Each patient is injected in the Pre-induction phase with 60mg IM Contramol, IV Metronidazole or Tinidazole and with 2grs. of Cefizox IV. The H2 receptor antagonist like ranitidine injection is also advisable.
Creation of Pneumoperitoneum.
- Check Veress needle before insertion.
- Check veress needle tip spring.
- Confirm that gas connection is functioning.
- Ensure flushing with saline does not block that needle.
- Make a small incision just above the umbilicus.
- Lift up abdominal wall and gently insert Veress needle till a feeling of giving way.
- Confirm position of needle by saline drop method.
- Connect CO2 tube to needle.
- Switch off gas when desired pneumoperitoneum is created & remove the Veress needle
Port location:
- A 10mm camera port is placed in the umbilicus; this position will vary according the build of the patient.
- A 5mm port is inserted between xiphoid process and umbilicus in the mid-line.
- A 5 mm port, is placed in the left lower quadrant.
Exposing the anterior wall of the stomach and identifying the site of tube insertion :
- Manipulate the stomach using two hand technique using atraumatic grasper to find the proper site of gastrostomy tube insertion.
- The site on the anterior wall of stomach is selected keeping in mind that gastrostomy tube should always be placed under no tension between the stomach and abdominal wall.
Insertion of Gastrostomy tube in the abdominal cavity:
- Insert a 5 mm trocar at the exact location of plan of gastrostomy on the anterior abdominal wall.
- Insert an Endo dissect instrument via the lower midline trocar into the newly inserted 5 mm port.
- Remove VERSAPORT 5 mm over the ENDO DISSECT instrument.
- Grasp the distal end of the gastrostomy tube outside the intra-abdominal cavity with ENDO DISSECT instrument and pulled inside.
- Clamp the gastrostomy tube outside the intra-abdominal cavity to prevent air leak.
Insertion of Gastrostomy Tube in the Stomach
- Grasp the anterior abdominal wall with an atraumatic grasper exactly proximal to the site where you want to create gastrostomy.
- Make a gastrostomy hole of 5mm size using the ENDO SHEARS instrument.
- Grasp the gastrostomy tube and insert into the stomach.
- Verify the catheter is in the stomach.
- Do not create a sub-mucosal tunnel.
Securing the Gastrostomy
- Sew purse string suture around the insertion site of the catheter into the stomach.
- It is wise to double the purse string so that there should not be any leak and there should not be any rough area.
- Sew the purse on the anterior abdominal wall to secure the gastrostomy properly.
- Always place additional sutures to secure the catheter and stomach onto the abdominal wall.
Ending of the operation.
- Examine the abdomen for any possible bowel injury or haemorrhage.
- Remove the Instrument and then port.
- Remove telescope leaving gas valve of umbilical port open to let out all the gas.
- Close the wound with Suture.
- Use vicryl for rectus and Un-absorbable intra-dermal or Stapler for skin.
- Apply adhesive sterile dressing over the wound.
Gastrostomy tube feeding may be started from the second day. Patient may be discharged 3rd or 4th days after operation if every things goes well. The patient may have slight pain initially but usually resolves. The patient having any complain should be examined endoscopically.
Minimal Access Surgeon




