Nina Irawati
Department of Surgery Awalbros Hospital
Jalan Gajahmada Kav I Batam Indonesia
Published in World Journal of Laparoscopic Surgery Please log on the //www.wjols.com to get this issue
Abstract
Background: We report our two initial experiences in the treatment of thyroid disease with Endoscopic Tyhroidectomy. Minimally Invasive Video-Assisted Technique (MIVAT) was initially introduced by Miccoli. The modification was made by using axillary and breast approach with CO2 insufflation.
Method: Patient young woman, with 5 cm right lobe thyroid disease suspected benign. From physical examination, sonography , and FNAB findings were categoized as benign case. Tyhroid function test within normal limit. She was operated with endoscopic right lobectomy. The procedure was carried out through incision of 5-10 mm axillary and breast approach. The right lobectomy procedure was performed by dedicated instrument. No drain needed. The pathology result was follicular carcinoma, so further treatment needed. Other patient, woman with 4 cm right lobe thyroid cyst. FNAB proved benign, was operated with the same procedure and pathology result was benign cyst.
Result: Duration of first operation was 300 minutes and the second one was 120 minutes, minimal blood loss, and no major complication. Patients were discharged 24 hour after operation. Cosmetic result and post operative pain were excellent. Slight swelling on their necks was found and reduced after 48 hours. Pain around shoulder until day-7 pos operative and significantly disappeared after 10 days.
Conclusion: We reported two cases with were operated by endoscopic right lobectomy as a safe, reproducible technique with an indication in a minority of patients candidates to thyroidectomy and is characterized by a better postoperative discomfort. The duration of operation would be a curve learning for each surgeon who wishes to perform it.
Keyword: endoscopic thyroidectomy, axillary -breast approach:
Neck surgery is one of the newest and most interesting application of minimally invasive surgery technique in thyroid surgery, particularly with regard to eliminating the unattractive scars.1,2. It is well known that conventional thyroidectomy allows for prompt postoperative recovery. In some clinical settings, it is performed as an outpatient procedure. Findings have shown that video-assisted and endoscopic procedure for thyroid surgery have some advantages over conventional surgery in term of cosmetic result and postoperative recovery. These results support the development of endoscopic and video-assisted thyroid surgery. It should be emphasized that these procedures are technically demanding and require a surgical team skilled in both endocrine and endoscopic surgery. This is particularly true for some endoscopic techniques such as endoscopic thyroidectomy by breast or axillary approach. The endoscopic and video-assisted procedure requires a significant learning period, which can be time consuming especially at the beginning of a surgeon’s experience.3. Minimal-access thyroid surgery was conceived primarily in Europe and Asia.1 Endoscopic neck surgery for the parathyroid and thyroid was developed by Gagner and Huscher in 1996 and 1997, respectively. Since then, various methods including axillary, breast, and anterior chest approaches have been introduced by many surgeons. The use of endoscopic for complete thyroidectomy has been viewed with concern, although many surgeons have regarded benign thyroid disease as an indication for endoscopic surgery. 4-7.

Case illustration I
Women, 32 years old with lump on right anterior neck since a year ago. The lump was not tender, meat ball size, not getting bigger, skin upon was not redness. No other lump around her neck and other part of the body. No other people in her community had the same symptom.
From physical examination, general condition was good. Local status showed lump on anterior neck region, no redness, size around 5cm in diameter , firm, not tender, moved upward when swallowing, no lymph node enlargement around neck. Laboratory finding within normal limit. Sonography and FNAB findings were concluded as benign case. She was operated right lobectomy endoscopically. Pathologic result was follicular carcinoma. Futher treatment needed and she is now prepared for completion thyroidectomy endoscopically.
Case illustration II
Women, 34 years old with lump on right anterior neck since 6 month ago. The lump was not tender, meat ball size, not getting bigger, skin upon was not redness. No other lump around her neck and other part of the body. No other people in her community had the same symptom. >General condition was good. Local status showed lump on anterior neck region, no redness, size around 4cm in diameter , firm, not tender, moved upward when swallowing, no lymph node enlargement around neck. Laboratory finding within normal limit. Sonography and FNAB findings were concluded as benign cyst. She was operated right lobectomy endoscopically. Pathologic result was benign cyst of thyroid.
Method
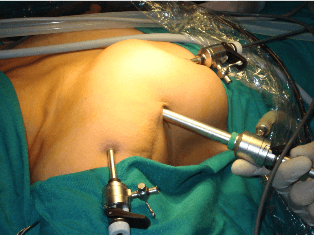
Our first two cases report, using axillary-breast approach similar to Tran Ngoc Luong technique to perform endoscopic right lobectomy. Under general anesthesia, those patients were placed in the supine position with the neck moderately extended. The port sites were identified. At first, 10 mm longitudinal incision was made at anterior axillary region. Then 5 mm incision circumareolar and shoulder. Then a vascular clamp was used to create the preliminary subfascial space. A 10 mm trochar was placed as the optical port. The operating space was maintained with O2 insufflation at a gas pressure of 10-11 mmHg. A 10 mm 0 degree endoscope was inserted. Under its guidance, we inserted other 5 mm trochar respectively. The subcutaneous tunnel was further enlarged with bipolar and hook equipment. The lateral border of sternocleidomastoideus was dissected and omohyoid was moved upward. The thyroid gland was exposed. The inferior and superior thyroid arteries were divided using harmonic scalpel. The parathyroid and RLN were routinely identified and preserved. The gland was dissected by harmonic as well.

Result
The duration of first operation was 300 minutes, with bleeding 75 cc. We didn’t have frozen section facility, so we had to wait for definitive pathology result. Post operatively, there was slightly edema on the neck, pain around shoulder, and no hoarseness (RLN paralysis) . Calcium level was normal. After 7 day post operation, the pain and edema reduced. Because the pathology result was follicular, the patient needs completion operation after endoscopically. The second patient was operated in 120 minutes with bleeding 30 cc. Post operatively was bruise on the right shoulder, no hoarseness , and slightly pain around shoulder. After 7 day post operation, she had no complaint.
Discussion
The history began with the initial experience conducted with MIVAP (Minimally Invasive Video-assisted Parathyroidectomy) led some authors to perform the same surgical approach for the thyroidectomy. The first idea that moved to MIVAT (Minimally Invasive Video-assisted Thyroidectomy) was the better cosmetic result (an incision of 1,5-2 cm). Micolli introduced this technique as a three-part procedure starting with an open technique, then followed by endoscopic component and then completed in an open fashion. According to some data in the literature, any surgeons approaching the MIVAT technique must carefully consider that at the beginning of his or her experience, the procedure will be significantly longer than the standard operation. From then, endoscopic thyroidectomy can be divided in two type, with CO2 insufflation or gasless. Others classified as video-assisted and total endoscopic.1,7,8
Total endoscopic thyroidectomy is a more sophisticated variation of minimally invasive thyroid. Using special instrument and technique, part or all of the thyroid gland can be removed through small puncture site, avoiding any incision on the neck whatsoever. In this technique, the skin overlying the collarbone is lifted from the underlying muscle and laparoscopic techniques are used to create a working space.8
Various approaches have been devised and improved further to fulfill this goal, mainly including the cervical approach, anterior chest approach, axillary and breast approach. However, none of these approaches is exclusively advantageous and universally accepted. The cervical approach and anterior chest approach are minimally invasive, but not cosmetically excellent. The axillary and breast approaches have maximized cosmesis, but meanwhile cause much invasiveness. Furthermore, the axillary approaches is not suitable for bilateral manipulation and even more technically challenging with abnormal anatomic vision. Therefore, an axillary-bilateral-breast approach (ABBA) has been developed, which is actually a combination of the procedure. In comparison, ABBA permits bilateral exploration, more space for instrument use, and the removal of larger nodule. With this technique, the mean surgical time was 188 minute, mean blood loss was 53 ml, and mean hospital stay was 3,3 days. BABA (bilateral-axillary-breast approach) was introduced later and was claimed be easily applied for thyroid cancer as well.3,5,6,7,9 This technique now is even improved by using da vinci robotic system by Eun Lee et all6 which is useful in identification of anatomy and dissection during surgery. The endowrist function of the instrument is beneficial in doing complex tasks in difficult areas with limited access. The mean operating time without robotic was 165 minute and with robotic was 218,3 minute, but there is tendency of decrease in operation time. They also perform central node dissection and limited lateral node picking. Tran Ngoc Luong 10 in 2004 modified the technique by using axillary-breast-shoulder approach. Using the technique, they can do total and other bilateral procedure, including central neck dissection. The first operating time was 420 minute and significantly reduced by mean time for lobectomy is 15 minutes and total is 30 minutes now.
The first endoscopic surgery which was performed transcervically, was employed to treat a 3-mm moderately differentiated papilary microcarcinoma with focal capsular invasion in 1997. The use of a transcervical approach results in small operative scars in the neck. 4 After this attempt, Ohgami et al11 performed endoscopic via breast approach for thyroid adenoma 5-7 cm in diameter.Yamamoto et al 12 applied endoscopic by breast approach for Grave’s disease patients. Ikeda at al 13 applied anterior chest and axillary approach for follicular tumors, Graves’ disease and papillary microcarcinoma.
Generally, endoscopic thyroid surgery has been thought to be appropriate for benign thyroid disease. First, it was indicated for nodule not more than 3 cm, benign or low grade follicular lesion and papillary carcinoma. With contraindications were previous neck surgery, large goiter, locally metastase, previous neck irradiation, thyoiditis, and hyperthyroidism.14 These indications during the development of the technique then slightly changed. Some even can perform for nodule more than 5 cm, for Graves’ and thyroiditis. 4,10 The role of endoscopic for carcinoma still in debate. In other areas of oncologic surgery, such for gastric or colorectal carcinoma, minimally invasive laparoscopic surgery has been established through clinical experience and technical development. Similarly, endoscopic thyroid surgery can be used for malignant thyroid disease. BABA and Axillary-breast approach similar to Tran Ngoc Luong technique can be used as an appropriate method for treating thyroid malignancies.4,6,10 Kitano et al 15 reported treatment of thyroid cancer with anterior chest approach endoscopic surgery. The indications are as follow : age<45 years, tumor size<2cm, and no evidence of lymph node metastase or local invasion. Micolli et al 16 showed that the completeness obtained with MIVAT for thyroid cancer not exceeding 3,5 cm in diameter is similar to that obtained with open surgery. As experience accumulates and more technique are developed, the indication in cases of thyroid malignancy can be expanded.4,6
Postoperative complication such as hypocalcemia, recurrent laryngeus nerve (RLN) paralysis, bleeding, infection, and pain. 4,5 Others as a complication of using CO2 insufflation are hypercapnia, subcutaneous emphysema, and severe tachycardia.5,17 Gottlieb et al18 reported severe increases in PaCO2, subcutaneous emphysema, and severe tachycardia by applied insufflations at relatively high pressure (15-20 mmHg) , whereas Ochiai et al 17 and Ohgami et al 11 reported only minimal emphysema with use of low pressure C02 insufflation (6mmHg).Tran Ngoc Luong technique used 10-11 mmHg insufflations of CO2 without severe complication appeared. The study of the appropriate pressure should be used still under observation.10 According to the literature, the conversion rate varies from 0-13%. The reason include malignant histological result, bleeding, difficulty of dissection, size of nodule, and thyroiditis. In some reports, 5-11% patients even required a second operation for definitive malignant pathological result.6 We performed our first case using axillary-breast approach similar to Tran Ngoc Luong technique. We didn’t find any difficulty in identifying the anatomy during operation, so we didn’t convert to open method. The operation time took relatively faster than the first operation which Tran Ngoc Luong did. There was minimal blood loss and no major complication found including the effect of CO2 insufflation. This technique was safe and feasible to perform. It provides excellent view of vital structure and has advantage over open method cosmetically, although it has learning curve. As we get more familiar, the shorter operating time will be and also extending indication for endoscopic thyroid surgery. We proved it with our second patient who was operated faster and with minimal blood loss.
Conclusions
Since its introduction and establishment in 1997, endoscopic thyroidectomy has yet to become a standard procedure. Thus this procedure will provide another surgical choice for patients with thyroid tumors and carcinoma.
References
- El-Labban GM. Minimally Invasive Video-Assisted Thyroidectomy : A Single-Blinded, Randomized Trial. The Internet Journal of Surgery 2010 ; volume 22 (number 2)
- Bellantone R, Pio Lombardi C, Bossola M, et al.. Video-Assisted vs Conventional Thyroid Lobectomy A randomized Trial. Arch Surg 2002; 137: 301-4
- Gal I, Solymosi T, Szabo Z, et al. Minimally Invasive Video-Assisted Thyroidectomy and Conventional Thyroidectomy :A-Prospective Randomized Study. Surg Endosc 2008; 22: 2445-9
- Seung Chng Y, Ho Choe J, Ho Kang K., et al. Endoscopic Thyroidectomy for Thyroid Malignancies: Comparison with Conventional Open Thyroidectomy. World J Surg 2007; 31: 2302-6
- Lai Park Y, Kon Han W, Gila Bae W. 100 Cases of Endoscopic Thyroidectomy. Surg Laparosc, Endosc & Percutan Tech 2003; 13 (1) : 20-25
- Eun Lee K, Rao J, Kyu Youn Y, et al. Endoscpic Thyroidectomy with the da-Vinci Robot System Unsing the BABA Technique- Our Initial Experience. Surg Laparosc, Endosc & Percutan Tech 2009; 19 (3): e71-5
- Lei Wang Y, Yong Zhang G, Xin Wang K.Endoscopic Thyroidectomy by A-Modified Anterior Chest Approach : A- single institution’s 5-year experience. Min Inv Therapy 2009 ; 18: 297-301
- Minimally Invasive Thyroid Surgery. Available from : www.thyroidectomy.com
- Barlehner E, Benhidjeb T. Cervical Scarless Endoscopic Thyroidectomy: Axillo-Bilateral-breast Approach (BABA). Surg Endosc 2008; 22: 154-7
- 10.Ngoc Luong T. Open and Endoscopic Thyroidectomy. Paper Lecture August 2009
- Ohgami M, Ishii S, Arisawa Y,et al. Scarless Endoscopic Thyroidectomy: Breast Approach for Better Cosmesis. Surg Laparosc Endosc Percutan Tech 2002; 21: 2166-71
- Yamamoto M, Sasaki A, Asahi H, et al. Endoscopic Subtotal Thyroidectomy for Patients with Graves’ Disease. Surg Today 2001; 31: 1-4
- Ikeda Y, Takami H, Sasaki Y. Comparative Study of Thyroidectomies: Endoscopic Surgery vs Conventional Open Surgery. Surg Endosc 2001; 16: 1741-5
- Del Rio P, Sommaruga L, Ferreri G, et al. Preliminary Experience in Minimally Invasive Videoassisted Thyroidectomy (MIVAT). Acta Bio 2006; 77: 27-9
- Kitano H, Fujimura M, Kinoshita T, et al. Endoscopic Thyroid Resection Using Cutaneous Elevation in Lieu of Insufflation. Surg Endosc 2002; 16: 88-91
- Miccoli P, Berti P, Raffaelli M, et al. Comparison between Minimally Invasive Video-assisted Thyroidectomy and Conventional Thyroidectomy: a prospective randomized study. Surg 2001; 130: 1039-43
- Ochiai R, Takeda J, Noguchi J. Subcutaneous Carbon Dioxide Insufflation Does Not Cause Hypercarbia During Endoscopic Thyroidectomy. Anesth Analg 2000; 90: 760-2
- Gottlieb A, Sprung J, Zheng XM, et al. Massive Subcutaneous Emphysema and Severe Hypercarbia in a Patient During Endoscopic Transcervical Parathyroidectomy using Carbon Dioxide Insufflation. Anesth Analg 1997; 84: 1154-6





