BASIC INFORMATION
Date & Time: June 6, 2026, 8:26 PM Indian Standard Time
Lecture Handout Prepared from the Teaching Session by: Dr. R. K. Mishra
SUMMARY
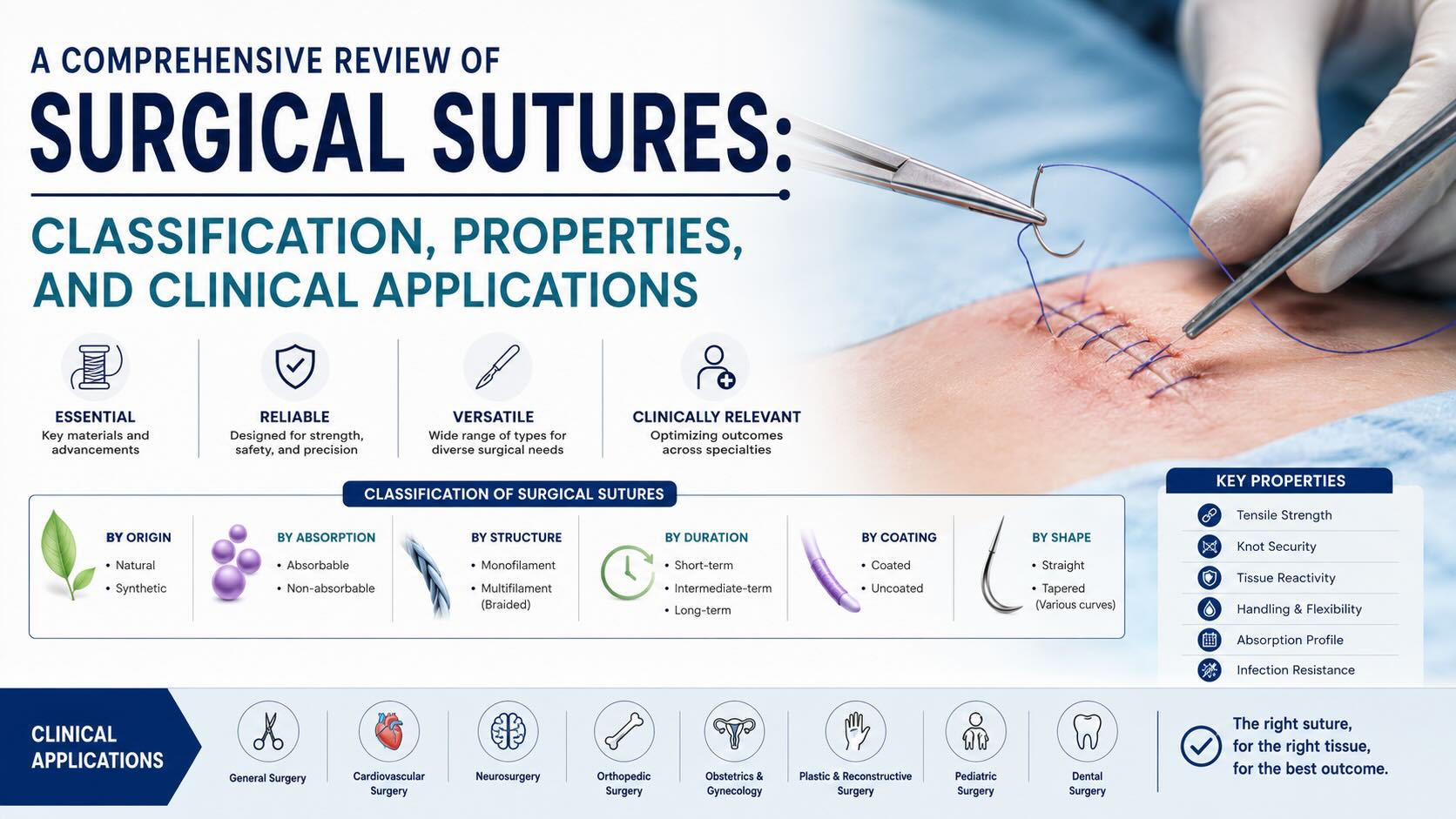
This document provides a comprehensive overview of surgical sutures, intended for postgraduate trainees in surgery and gynecology. The content is structured to facilitate a clear understanding of suture classification, materials, and clinical applications. Key topics include the standardized sizing system (from size 6 down to 11-0), the fundamental distinction between absorbable and non-absorbable materials, and the structural differences between monofilament and multifilament sutures. The lecture details the physical properties associated with each type, such as tissue drag, knot security, memory, and potential for harboring infection. It reviews common suture materials including gut, Monocryl, PDS, Prolene, Vicryl, and Silk, outlining their composition, characteristics, and typical surgical uses. The handout also covers the primary classifications of surgical needles—taper point, blunt point, conventional cutting, and reverse cutting—and concludes with an analysis of suture package labeling to aid in rapid and accurate identification in the operative setting.

KEY KNOWLEDGE POINTS
-
Standardized Suture Sizing System
-
Classification: Absorbable vs. Non-absorbable
-
Classification: Monofilament vs. Multifilament
-
Properties and Clinical Implications of Different Suture Types
-
Common Suture Materials and Their Applications
-
Surgical Needle Anatomy and Classification
-
Interpretation of Suture Packaging
INTRODUCTION
The selection of appropriate suture material is a fundamental skill in surgery, critical to achieving optimal wound healing and successful patient outcomes. The term "suture" refers to both the material used to ligate vessels or approximate tissues and the act of applying it. A vast array of suture materials exists, each with distinct properties tailored to specific surgical scenarios. A surgeon's choice is guided by the biological characteristics of the tissue being repaired, the required tensile strength and duration of wound support, the suture's handling properties, and its interaction with host tissues. A thorough understanding of suture classification, from sizing and absorption profile to filament structure, is therefore essential for the practicing surgeon. This review aims to systematically organize and clarify these concepts for postgraduate learners.
LEARNING OBJECTIVES
-
Describe the evolution and current standard of the surgical suture sizing system, including the "aught" or "zero" notation.
-
Differentiate between absorbable and non-absorbable sutures, providing clinical examples for the appropriate use of each.
-
Compare and contrast the properties of monofilament and multifilament sutures, including memory, knot security, tissue drag, and risk of infection.
-
Identify the composition, characteristics, and primary clinical applications of common suture materials such as Gut, Monocryl, PDS, Prolene, Vicryl, and Silk.
-
Classify the four main types of surgical needles and explain the rationale for their use in different tissue types.
-
Accurately interpret the information provided on a standard suture package.
CORE CONTENT
1. Suture Sizing
The United States Pharmacopeia (USP) provides a standardized sizing system for surgical sutures, which denotes the diameter of the suture material.
-
Historical Sizing: The initial system comprised sizes 1 through 6, with size 1 being the smallest and size 6 the largest. Size 1 was approximately 0.43 mm, and size 6 was nearly 1 mm in diameter.
-
Development of Finer Sutures: As manufacturing technology advanced, sutures smaller than size 1 were developed. This led to the introduction of size 0, followed by multiple zero or "aught" sizes.
-
Modern Sizing Convention:
-
Sutures larger than size 0 are denoted by integers (e.g., 1, 2, 3, up to 6), where a larger number indicates a larger diameter.
-
Sutures smaller than size 0 are denoted by a number followed by a hyphen and a zero (e.g., 2-0, 3-0, 4-0). In this "aught" system, a higher prefix number indicates a smaller diameter.
-
The range extends from the largest sizes (e.g., size 6) down through 1, 0, 2-0, 3-0, and so on, to the finest sutures, such as 11-0.
-
For context, a 7-0 suture has a diameter comparable to that of a human hair. An 11-0 suture is approximately one-third the diameter of a human hair and is used in microsurgical procedures.
-
2. Suture Classification by Absorption Profile
Sutures are fundamentally categorized based on their behavior within biological tissues over time.
2.1. Absorbable Sutures
These sutures are broken down and metabolized by the body over time through enzymatic degradation or hydrolysis. They provide temporary wound support until the tissue has healed sufficiently to withstand stress.
-
Indications:
-
Approximation of tissues deep within the body where suture removal is not feasible (e.g., closing fascial layers, peritoneum).
-
Suturing of rapidly healing tissues with good vascularity (e.g., oral mucosa, subcutaneous tissue).
-
Cutaneous closure where the patient's return for suture removal is undesirable or unlikely.
-
-
Examples: Plain Gut, Chromic Gut, Vicryl (Polyglactin 910), Monocryl, PDS.
2.2. Non-Absorbable Sutures
These sutures are made of materials that resist enzymatic degradation and remain permanently encapsulated within the body's tissues, or they are removed after adequate healing has occurred.
-
Indications:
-
Tissues requiring prolonged or permanent mechanical support.
-
Anastomosis of high-pressure structures, such as arteries, where premature suture degradation could lead to catastrophic failure.
-
Repair of slowly healing tissues with poor vascularity (e.g., tendons, ligaments).
-
Skin closure where sutures will be removed postoperatively.
-
Fixation of prosthetic materials, such as surgical mesh for hernia repair.
-
-
Examples: Prolene, Ethilon (Nylon), Silk, Ethibond, Surgical Steel.
3. Suture Classification by Filament Structure
The physical construction of the suture thread significantly influences its handling characteristics and biological interaction.
3.1. Monofilament Sutures
These consist of a single, solid strand of material.
-
Properties:
-
Smooth Surface: Glides easily through tissue, causing minimal tissue trauma or drag. This is advantageous in delicate tissues like blood vessels.
-
Reduced Infection Risk: The absence of interstices (nooks and crannies) makes it difficult for bacteria to colonize the suture, reducing the risk of suture-line infections.
-
Memory: Tend to retain the shape they held in the package ("memory" or "recoil"). This property can make handling and knot tying more challenging.
-
Knot Security: Knots may be less secure due to the smooth surface and memory, often requiring additional throws to prevent slippage.
-
-
Examples: Monocryl, PDS, Prolene, Ethilon.
3.2. Multifilament Sutures
These are composed of multiple small threads that are braided or twisted together.
-
Properties:
-
Pliability and Flexibility: Generally have low memory, are easy to handle, and drape well.
-
High Knot Security: The braided texture creates friction, allowing for secure knots that are less likely to slip.
-
Increased Tissue Drag: The rougher surface can cause more friction and trauma when pulled through tissue compared to a monofilament.
-
Potential for Infection: The interstices between filaments can provide a nidus for bacteria, shielding them from host immune defenses. Therefore, they are relatively contraindicated in the presence of active infection.
-
-
Examples: Vicryl, Silk, Ethibond.
4. Common Suture Materials
4.1. Absorbable
-
Plain Gut (Catgut): A natural monofilament derived from purified collagen of bovine or ovine intestines. It is absorbed rapidly (within days) via enzymatic proteolysis. Used for rapidly healing tissues with good blood supply (e.g., oral mucosa). Packaged in an alcohol solution.
-
Chromic Gut: Plain gut treated with chromium salts to increase its tensile strength and slow its absorption rate to a few weeks. It shares the properties of plain gut but provides longer wound support.
-
Monocryl: A synthetic absorbable monofilament suture. Often used for soft tissue approximation and ligation. It has properties similar to chromic gut but is synthetic.
-
PDS (Polydioxanone): A synthetic absorbable monofilament suture providing extended wound support. The package label explicitly identifies it as "monofilament" and "absorbable."
-
Vicryl (Polyglactin 910): A synthetic absorbable multifilament (braided) suture. It is one of the most widely used sutures for general soft tissue approximation. It handles well and has excellent knot security. Typically dyed violet, but also available undyed (white).
4.2. Non-Absorbable
-
Prolene (Polypropylene): A synthetic non-absorbable monofilament suture. It is known for its extremely low tissue reactivity and high tensile strength, lasting indefinitely in the body. It is characteristically bright blue. Ideal for vascular anastomoses, cardiovascular surgery, and hernia mesh fixation.
-
Silk: A natural non-absorbable multifilament (braided) suture derived from silkworm fibers. It has excellent handling and knotting characteristics but is known to elicit a significant inflammatory response. It should not be used in the presence of infection. Often used for securing surgical drains. Typically dyed black.
-
Ethilon (Nylon): A synthetic non-absorbable monofilament suture. Commonly used for skin closure.
5. Surgical Needle Classification
Surgical needles are designed to carry suture through tissue with minimal trauma. They are classified primarily by their point geometry.
-
Taper Point: The needle body is round and tapers to a sharp point. It is used for easily penetrated tissues like peritoneum, viscera, and vascular structures, as it pierces and spreads tissue without cutting.
-
Blunt Point: The needle body is round, and the tip is blunted. It is designed to dissect through friable tissue (e.g., liver, kidney) without cutting, reducing the risk of hemorrhage.
-
Conventional Cutting: The needle body is triangular in cross-section with three cutting edges. The third cutting edge is on the inner (concave) curvature of the needle. Used for tough tissues like skin. A potential disadvantage is that the upward-facing cut may promote tissue tear-out.
-
Reverse Cutting: The needle body is also triangular, but the third cutting edge is located on the outer (convex) curvature. This design is stronger and less likely to cause tissue to tear out when tension is applied, making it a preferred choice for tough tissues like skin and fascia.
6. Interpretation of Suture Packaging
Suture packets are standardized to provide essential information at a glance.
-
Suture Size (USP): The most prominent feature (e.g., 5-0).
-
Suture Name and Material: Brand name (e.g., Ethilon) and generic material (e.g., Polyamide 6).
-
Suture Length: Given in inches or centimeters (e.g., 18 inches).
-
Needle Information:
-
Needle Code: A manufacturer-specific code (e.g., PS-2).
-
Needle Type: A silhouette and description (e.g., Reverse Cutting).
-
Needle Dimensions: A life-sized diagram showing curvature and length.
-
Number of Needles: Usually one, but double-armed sutures will show two needles.
-
-
Absorption Profile: Clearly states "Absorbable" or "Non-Absorbable."
-
Expiration Date: Mandatory for ensuring sterility and material integrity.
SURGICAL PEARLS
-
Monofilament sutures require extra throws (e.g., five or six) to ensure knot security due to their inherent memory and smooth surface.
-
Never use multifilament sutures, particularly Silk, in a known or suspected infected field. The braided structure can harbor bacteria and create a persistent septic focus.
-
When suturing delicate vascular tissue, a monofilament suture (e.g., Prolene) is preferred to minimize tissue drag and trauma.
-
Always check the expiration date on every suture packet before opening it onto the sterile field.
-
For laparoscopic or microscopic surgery where ambient light is low, colored sutures (e.g., blue Prolene, violet Vicryl) are significantly easier to visualize than undyed sutures.
COMPLICATIONS AND THEIR MANAGEMENT
-
Intraoperative:
-
Tissue Tear-out: Can occur with cutting needles in friable tissue or if excessive tension is applied. Managed by re-suturing with a more appropriate needle (e.g., taper) or technique.
-
Suture Breakage: May occur if excessive force is applied. Requires removal of the broken segment and replacement.
-
-
Early Postoperative:
-
Suture Line Dehiscence: Can result from premature absorption, insecure knots, or excessive tissue tension. Requires urgent re-exploration and re-closure.
-
Suture-Related Infection: More common with multifilament sutures. Manifests as erythema, purulent discharge, and inflammation. Managed with antibiotics and, if a non-absorbable suture is the nidus, potential removal.
-
-
Late Postoperative:
-
Suture Granuloma: An inflammatory reaction to retained suture material, particularly natural fibers like Silk. May present as a palpable nodule. Management may involve observation or excisional biopsy if symptomatic.
-
Suture Sinus: A tract that forms from a deep, often infected, non-absorbable suture to the skin surface. Definitive management requires surgical excision of the suture and the entire tract.
-
MEDICOLEGAL AND PATIENT SELECTION CONSIDERATIONS
-
Informed Consent: While specific suture types are not typically detailed, discussion of wound closure and potential complications (infection, scarring, dehiscence) is a standard component of consent.
-
Off-Label Use: Using a suture for a purpose not specified by the manufacturer should be based on sound clinical judgment and experience.
-
Patient Factors: The choice of absorbable versus non-absorbable skin sutures may be influenced by the patient's ability and willingness to return for removal. In pediatric or non-compliant patients, absorbable sutures may be preferred to obviate the need for a removal visit.
-
Documentation: The type and size of suture used, particularly for permanent implants like mesh or vascular grafts, should be clearly documented in the operative report.
SUMMARY AND TAKE-HOME MESSAGES
-
Suture selection is a critical surgical skill that directly impacts wound healing. The choice depends on tissue type, required support duration, and handling needs.
-
Sutures are classified by size (aught system), absorption profile (absorbable/non-absorbable), and structure (monofilament/multifilament).
-
Monofilaments glide smoothly but have memory and require more throws for knot security. Multifilaments handle well and hold knots securely but can harbor bacteria.
-
Common synthetic sutures like Vicryl (absorbable multifilament) and Prolene (non-absorbable monofilament) are workhorses in modern surgery.
-
Understanding needle anatomy (taper vs. cutting) is crucial to minimize tissue trauma and ensure suture placement is effective and secure.
MULTIPLE CHOICE QUESTIONS (MCQs)
-
Which of the following suture sizes has the largest diameter?
a) 3-0
b) 0
c) 2
d) 5-0
-
A surgeon is performing an anastomosis of the femoral artery. Which suture characteristic is most critical for this procedure?
a) Rapid absorption
b) Non-absorbable and monofilament
c) Multifilament and absorbable
d) High memory
-
What is the primary disadvantage of using a multifilament suture like Silk?
a) Poor knot security
b) High degree of memory
c) Potential to harbor bacteria
d) Causes minimal tissue drag
-
A surgeon requests "Polyglactin 910." Which suture should be provided?
a) Prolene
b) PDS
c) Monocryl
d) Vicryl
-
Which suture property is described as the tendency to retain its packaged shape and spring back?
a) Pliability
b) Memory
c) Knot strength
d) Capillarity
-
When suturing the liver, a highly friable organ, which type of needle point is most appropriate to minimize trauma?
a) Reverse cutting
b) Conventional cutting
c) Taper
d) Blunt
-
A suture with a diameter approximately equal to a human hair would be designated as:
a) 2-0
b) 1
c) 7-0
d) 11-0
-
Which of the following is a natural, absorbable monofilament suture?
a) Silk
b) Ethilon
c) Chromic Gut
d) Vicryl
-
A surgeon is closing the skin on a patient who is unlikely to return for follow-up. Which suture is the most appropriate choice?
a) Prolene
b) Ethilon
c) Surgical Steel
d) Monocryl
-
A reverse cutting needle is distinguished by having its third cutting edge on the:
a) Inner concave curvature
b) Outer convex curvature
c) Tip of the needle only
d) Body of the needle shaft
-
Which suture is synthetic, non-absorbable, monofilament, and characteristically bright blue?
a) Vicryl
b) Prolene
c) Silk
d) PDS
-
A surgeon notes that a suture is braided and dyed violet. It is most likely:
a) Prolene
b) Chromic Gut
c) Vicryl
d) Silk
-
All of the following are characteristics of monofilament sutures EXCEPT:
a) Minimal tissue drag
b) Excellent knot security with few throws
c) Reduced risk of harboring bacteria
d) Presence of memory
-
For which clinical scenario would a non-absorbable suture be indicated?
a) Closing the oral mucosa after a tooth extraction
b) Subcutaneous closure in an abdominal incision
c) Repair of a flexor tendon in the hand
d) Ligation of a small subcutaneous blood vessel
-
What is the mechanism of absorption for synthetic sutures like Vicryl and PDS?
a) Enzymatic degradation
b) Phagocytosis
c) Hydrolysis
d) Encapsulation
-
Which of the following is a braided, non-absorbable suture derived from a natural source?
a) PDS
b) Ethilon
c) Silk
d) Monocryl
-
A surgeon repeatedly ties extra knots when using a specific suture. This suture is most likely:
a) A braided multifilament
b) A monofilament with high memory
c) A suture with low tensile strength
d) A rapidly absorbing suture
-
What does the "PS-2" on a suture package label refer to?
a) The suture size
b) The suture material
c) The specific manufacturer code for the needle
d) The length of the suture in inches
-
Why should silk suture not be used in the presence of infection?
a) It dissolves too quickly.
b) Its multifilament structure can serve as a nidus for infection.
c) It has poor knot security, leading to dehiscence.
d) It is a monofilament and cuts through tissue.
-
A conventional cutting needle is primarily used for which type of tissue?
a) Bowel
b) Blood vessels
c) Tough tissue like skin
d) Friable tissue like the spleen
Correct Answers: 1(c), 2(b), 3(c), 4(d), 5(b), 6(d), 7(c), 8(c), 9(d), 10(b), 11(b), 12(c), 13(b), 14(c), 15(c), 16(c), 17(b), 18(c), 19(b), 20(c)
MOTIVATIONAL MESSAGE FROM DR. R. K. MISHRA
True mastery in surgery is not found in the complexity of the procedure, but in the flawless execution of its fundamental steps. Dedicate yourself to perfecting the basics, for they are the foundation upon which every great surgical outcome is built.
My best wishes to all of you in your pursuit of surgical excellence. Continue to learn with passion and practice with precision.