BASIC INFORMATION:
Date & Time: May 25, 2026, 19:42:29 Indian Standard Time
Lecture Handout Prepared from the Teaching Session by: Dr. R. K. Mishra
SUMMARY:
This lecture provides a comprehensive overview of the laparoscopic insufflator, emphasizing its critical role in surgical safety. It details the instrument's function, moving beyond the misconception of it being a simple gas pump to explain its intelligence as a microprocessor-controlled device. The discussion covers the different types of insufflators, the significance of flow rates for various procedures (from basic gynecological diagnostics to advanced solid organ surgery), and the correct operational sequence to prevent errors. Key concepts such as preset pressure, actual pressure, flow rate, and total gas volume are explained through the "quadromanometric indicator" principle. The lecture uses clinical scenarios to interpret insufflator readings, enabling surgeons to differentiate between correct intraperitoneal placement, preperitoneal insufflation, and dangerous intravascular entry of the Veress needle. Special attention is given to safety features, alarm interpretation, and the rationale for managing flow rates to prevent complications like hypothermia. The session also addresses pediatric settings and the correct handling of CO2 cylinders.
KEY KNOWLEDGE POINTS:
-
The laparoscopic insufflator is the most critical safety instrument in laparoscopy, as its malfunction or misuse is often invisible.
-
Understanding the quadromanometric indicators (preset pressure, actual pressure, flow rate, and total gas volume) is essential for safe peritoneal access.
-
Modern insufflators have intelligent safety features, such as error detection for incorrect setup sequences (e.g., RTPD error).
-
Correct interpretation of the relationship between actual pressure and total gas volume can confirm the location of the Veress needle tip (intraperitoneal, preperitoneal, intravascular, or intraluminal).
-
High-capacity insufflators (e.g., 45 L/min) are necessary for advanced procedures with a high risk of bleeding, but routine use should be at a low flow rate (e.g., 6 L/min) to prevent hypothermia from excessive gas exchange.
-
Pulsatile flow during Veress needle insufflation is a safety feature for accurate pressure measurement and potential synchronization with diaphragmatic movements.
-
Specific modes for pediatric surgery, extraperitoneal procedures, and emergencies are available and should be utilized appropriately.
INTRODUCTION:
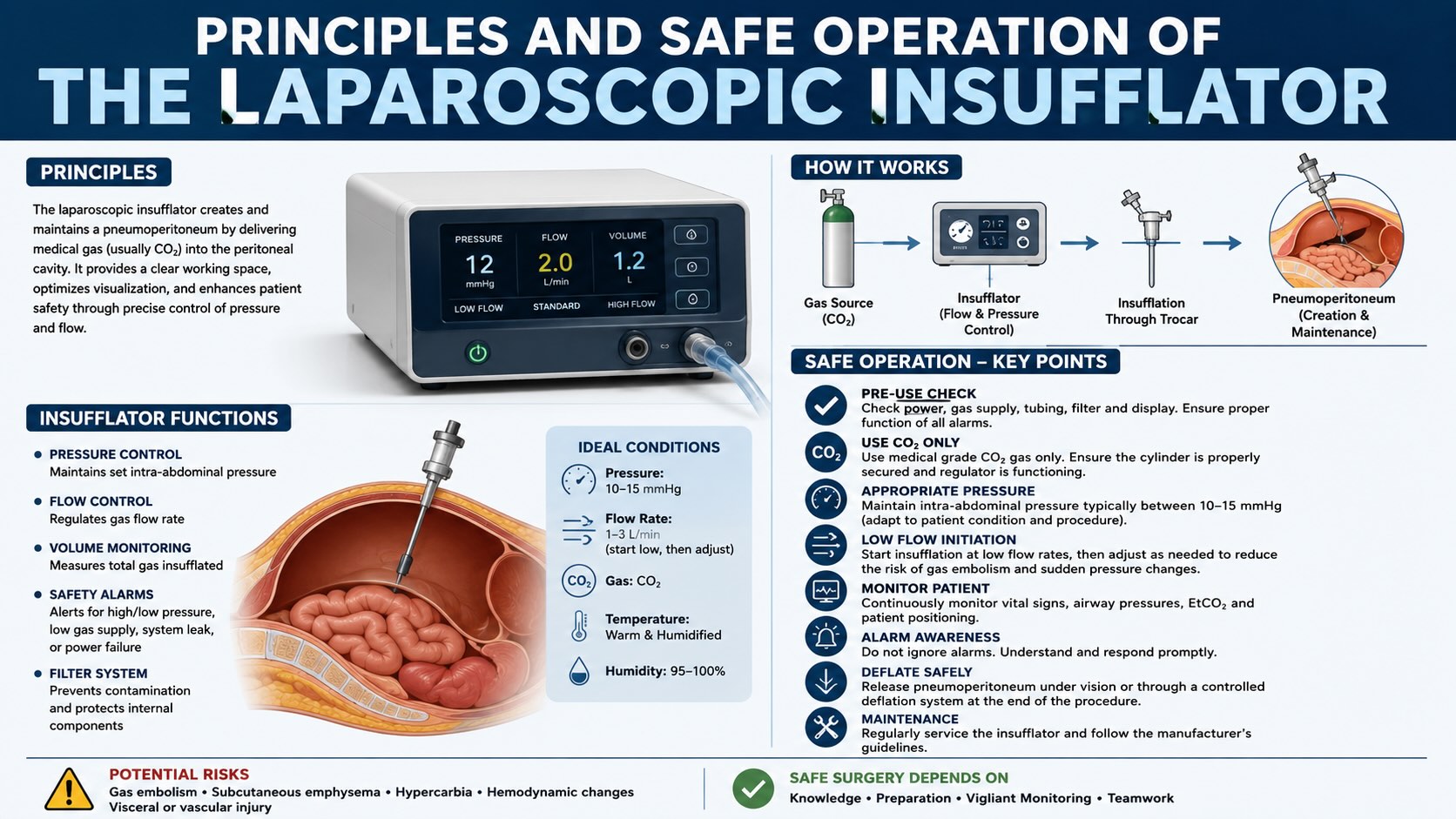
The creation and maintenance of a stable pneumoperitoneum are fundamental to laparoscopic surgery. The instrument responsible for this, the laparoscopic insufflator, is frequently misunderstood and underappreciated. While appearing to simply pump gas, the modern insufflator is a sophisticated, microprocessor-controlled device that provides critical real-time feedback about the intra-abdominal environment. A failure to correctly operate and interpret the data from the insufflator can lead to significant and often occult complications, including preperitoneal emphysema, gas embolism, and visceral injury. Therefore, a thorough understanding of its principles, functions, and safety mechanisms is not merely technical knowledge but a cornerstone of patient safety in minimally invasive surgery.
LEARNING OBJECTIVES:
-
To understand the fundamental operating principles of modern microprocessor-controlled laparoscopic insufflators.
-
To correctly interpret the quadromanometric indicators: preset pressure, actual pressure, flow rate, and total gas volume.
-
To recognize the signs of correct and incorrect Veress needle placement based on insufflator readings and prevent associated complications.
-
To apply appropriate flow rate settings for routine procedures, advanced surgeries, and pediatric cases to enhance safety and prevent complications like hypothermia.
-
To understand the common alarms and error messages of the insufflator and respond appropriately.
CORE CONTENT:
1. Principles of Insufflator Operation
1.1 Initial Setup and Safety Checks
The correct sequence of operation is critical. An incorrect setup can trigger safety lockouts in modern insufflators.
-
Correct Sequence: First, switch on the insufflator with the gas tubing disconnected from the patient cannula. This allows the machine to perform a self-test and purge any air trapped in the system (approximately 800 mL of gas from the cylinder to the tubing tip). The device will indicate "Device OK" upon successful completion.
-
Incorrect Sequence: Attaching the tubing to the cannula before powering on the insufflator. This traps air in the tubing, which could be insufflated into the patient. Modern insufflators may detect this as an error (e.g., "RTPD - Relay Transport Protocol Deactivated") and will not start the flow, preventing potential air embolism.
1.2 The Quadromanometric Indicators
The user interface of a modern insufflator typically displays four key parameters that must be constantly monitored.
-
Preset Pressure (Command Pressure): This is the intra-abdominal pressure limit set by the surgeon (e.g., 12-15 mmHg for standard adult laparoscopy). The insufflator’s primary goal is to achieve and maintain this pressure.
-
For extraperitoneal surgery (TEP hernia repair, axilloscopy), pressures up to 20 mmHg may be used.
-
For specific applications like subcutaneous space creation (breast augmentation), pressures may be set as high as 25 mmHg.
-
-
Actual Pressure (True Pressure): This is the real-time pressure measured at the tip of the insufflation tubing. This value provides the most crucial feedback regarding the location of the needle/trocar tip. Before insufflation, it should read zero.
-
Flow Rate: This panel has two components:
-
Set Flow Rate: The maximum flow rate the surgeon allows the machine to use (e.g., 1 L/min for Veress needle entry). This is not a constant flow but a ceiling.
-
Actual Flow Rate: The real-time rate at which gas is flowing into the abdomen. This rate is determined by the insufflator based on the "demand" needed to maintain the preset pressure. If there is no gas leak, the actual flow will be zero once the preset pressure is reached.
-
-
Total Gas Volume: This displays the cumulative volume of CO2 (in liters) used since the counter was last reset. It helps in assessing the progress of insufflation and detecting large, ongoing leaks. The counter can typically be reset to zero by pressing on the display.
2. Interpreting Insufflator Readings for Veress Needle Placement
The relationship between the actual pressure and the total gas volume consumed is the key to verifying correct needle placement.
2.1 Correct Intraperitoneal Placement:
A parallel relationship exists between the rise in actual pressure and the volume of gas insufflated.
-
Small, Muscular Patient: The abdomen is tight. A volume of 1.5 L may be sufficient to raise the pressure to 12 mmHg.
-
Grand Multiparous, Lax Abdomen: The abdomen is capacious. It may require 5-6 L of gas to achieve the same 12 mmHg pressure.
-
In both cases, the pressure rises steadily and proportionally as volume increases.
2.2 Incorrect Placement Scenarios:
-
Preperitoneal Insufflation: The preperitoneal space is a potential space with limited compliance.
-
Finding: The actual pressure rises very rapidly to meet the preset pressure after only a small volume of gas (e.g., 200-500 mL) is insufflated. The flow rate will then drop to zero or near zero.
-
Maximum Capacity: The preperitoneal space will typically accommodate a maximum of 1 L of gas at 12 mmHg pressure.
-
-
Intravascular Placement (e.g., in Vena Cava): This is a surgical emergency.
-
Finding: The insufflator delivers a continuous flow (e.g., 1 L/min), and a large volume of gas is consumed (e.g., >10 L), but the actual pressure fails to rise significantly, remaining low (e.g., 6 mmHg, reflecting central venous pressure).
-
Mechanism: CO2 is rapidly absorbed into the circulation. The human circulatory system can absorb CO2 at a rate of up to 1 L/min without immediate fatality. The pulsatile flow mode of the insufflator may also intermittently detect low pressure, misinterpreting it as an empty abdomen and continuing insufflation.
-
-
Intraluminal/Solid Organ Placement (Bowel, Stomach, Liver):
-
Finding: A small amount of gas is insufflated (e.g., <100 mL), and the actual pressure immediately rises to the preset level, causing flow to cease. This may be associated with unilateral or localized abdominal distension.
-
3. Flow Rate Management and Safety
3.1 Routine vs. Emergency Flow Rates:
-
High-Capacity Insufflators: Devices capable of 40-45 L/min flow are essential for advanced surgery (e.g., colorectal, bariatric, splenectomy) where rapid suctioning may be required during massive hemorrhage.
-
Routine Setting (Cruise Control): For routine surgery, it is a critical safety practice to limit the maximum flow rate to 6-10 L/min. This acts as a "cruise control."
-
Emergency Setting: In case of massive bleeding, the surgeon can override the low-flow setting (often via a long press of a button) to activate the maximum flow capacity (e.g., 40 L/min). This allows for aggressive suction and irrigation without losing the pneumoperitoneum.
3.2 Pediatric Mode:
Specialized pediatric settings must be used for children.
-
Pressure: The insufflator automatically defaults to a lower preset pressure (e.g., 8 mmHg).
-
Flow Rate: The flow rate is calculated based on the child's age: 0.1 L/min per year of age. After 10 years of age, adult settings are generally used.
4. CO2 Cylinder Handling
-
The CO2 cylinder must always be kept in an upright or slightly inclined position.
-
Placing the cylinder horizontally or upside down can cause liquid CO2 to enter the insufflator, potentially damaging its internal components.
SURGICAL PEARLS:
-
Always perform the "hanging drop test" as a clinical adjunct to insufflator readings when using a Veress needle.
-
Even when using an open (Hasson) technique, initiate insufflation at a low flow rate (1 L/min) to avoid an abrupt rise in intra-abdominal pressure, which can trigger a vasovagal response.
-
Listen to your insufflator. The alarms are designed to alert you to specific problems. Ignoring an alarm because you do not understand it is a common pathway to complications.
-
If you suspect preperitoneal insufflation after only 200-300 mL of gas, stop immediately and re-attempt access. Do not wait for a large preperitoneal space to develop, as this will make subsequent attempts more difficult.
-
During long procedures (>6 hours), periodically irrigate the intestines with warm saline to prevent desiccation from prolonged exposure to dry CO2 gas.
COMPLICATIONS AND THEIR MANAGEMENT:
-
Intraoperative
-
Gas Embolism: Suspected when there is a sudden drop in end-tidal CO2, hypotension, and cardiac arrhythmia after Veress needle placement with high gas consumption and low actual pressure. Management involves immediate cessation of insufflation, placing the patient in the left lateral decubitus (Durant's) position, and supportive care.
-
Hypothermia: Caused by high-flow leakage of cold, dry CO2 over a prolonged period. The rapid evaporation of peritoneal fluid leads to cooling of the splanchnic blood, which can cause ventricular fibrillation. Prevent this by limiting the maximum flow rate to 6-10 L/min during routine surgery and actively correcting any port site leaks.
-
Subcutaneous/Preperitoneal Emphysema: Diagnosed by a rapid rise in actual pressure with low gas volume. It is usually self-limiting but can make subsequent trocar placement difficult.
-
MEDICOLEGAL AND PATIENT SELECTION CONSIDERATIONS:
-
The surgeon is ultimately responsible for the safe operation of all equipment, including the insufflator. A thorough understanding of the device is mandatory.
-
The choice of insufflator capacity should match the complexity of the intended procedures. A low-flow (e.g., 6 L/min) insufflator is inadequate and unsafe for advanced procedures with a high risk of hemorrhage.
-
Documentation of insufflator settings and total gas volume used can be a valuable part of the operative record.
-
Failure to use specific safety features, such as pediatric mode in a child, could be considered a breach of the standard of care.
SUMMARY AND TAKE-HOME MESSAGES:
-
Treat the insufflator as an intelligent diagnostic tool, not just a gas pump. Its feedback is critical for safe abdominal access.
-
Master the interpretation of the four key indicators: preset pressure, actual pressure, flow rate, and total gas volume. The relationship between actual pressure and volume is paramount.
-
Always use a "cruise control" approach: set the maximum flow rate to a low, safe level (6-10 L/min) for routine work, and only activate high flow during a true emergency like major hemorrhage.
-
A rapid rise in actual pressure with minimal gas volume suggests preperitoneal placement. A failure of actual pressure to rise despite high gas volume suggests a major leak or a dangerous intravascular placement.
MULTIPLE CHOICE QUESTIONS (MCQs):
-
What is the correct initial step when setting up a modern laparoscopic insufflator?
a) Attach the tubing to the Veress needle and then switch on the machine.
b) Switch on the machine with the tubing attached to the cylinder but open to the air.
c) Set the desired pressure to 15 mmHg before powering on the device.
d) Connect the tubing to the patient cannula and then turn on the power.
-
A surgeon sets the preset pressure to 12 mmHg and the set flow rate to 1 L/min. During initial insufflation, the actual pressure reads 6 mmHg, and the total gas volume used is 12 liters. The abdomen is not distended. Where is the tip of the Veress needle most likely located?
a) In the preperitoneal space.
b) In the stomach.
c) In the vena cava.
d) The tubing has a minor leak.
-
During Veress needle insertion, the actual pressure rapidly rises to 12 mmHg after only 400 mL of CO2 has been insufflated. The flow rate drops to almost zero. This most likely indicates:
a) Correct intraperitoneal placement in a small patient.
b) Preperitoneal insufflation.
c) Intravascular insufflation.
d) Placement within the lumen of the small bowel.
-
Why do modern insufflators use a pulsatile flow mode during Veress needle insufflation?
a) To decrease patient pain during insufflation.
b) To allow the machine to accurately sense the static intra-abdominal pressure between gas pulses.
c) To conserve CO2 gas.
d) To heat the gas before it enters the abdomen.
-
What is the primary reason for limiting the maximum insufflation flow rate to 6-10 L/min during routine laparoscopy, even with a high-capacity (45 L/min) machine?
a) To prevent over-distension of the abdomen.
b) To minimize the cost of CO2 gas.
c) To prevent severe hypothermia from high-volume gas exchange.
d) To reduce wear and tear on the insufflator.
-
In which of the following clinical scenarios is a high-capacity (e.g., 45 L/min) insufflator most essential?
a) Diagnostic laparoscopy for infertility.
b) Laparoscopic tubal ligation.
c) Laparoscopic splenectomy.
d) Totally extraperitoneal (TEP) hernia repair.
-
A surgeon is performing a laparoscopic procedure, and a large port site leak develops. The 40 L/min insufflator compensates, maintaining pneumoperitoneum. What is the most significant life-threatening risk to the patient if this high-flow leak continues for an extended period?
a) Gas embolism.
b) Hypercarbia.
c) Visceral desiccation.
d) Hypothermia leading to ventricular fibrillation.
-
The insufflator display shows the preset pressure at 12 mmHg, the actual pressure at 12 mmHg, and the actual flow rate at 0 L/min. What does this indicate?
a) The insufflator has malfunctioned.
b) There is an occlusion at the tip of the cannula.
c) The desired pneumoperitoneum has been achieved and there is no leak.
d) The CO2 cylinder is empty.
-
What is the recommended maximum flow rate for a 4-year-old child undergoing laparoscopy?
a) 1.0 L/min
b) 0.1 L/min
c) 0.4 L/min
d) 4.0 L/min
-
The term "preset pressure" on an insufflator refers to:
a) The pressure inside the CO2 cylinder.
b) The real-time pressure inside the patient's abdomen.
c) The maximum pressure limit set by the surgeon.
d) The pressure required to open the insufflator valves.
-
An "RTPD" or similar error message appears when an insufflator is switched on with the tubing already attached to the patient cannula. This safety feature primarily prevents:
a) Insufflation of room air into the patient.
b) Damage to the insufflator's pressure sensor.
c) Over-pressurization of the abdomen.
d) Inaccurate measurement of total gas volume.
-
A surgeon observes that the graph of "Actual Pressure" versus "Total Gas Volume" is diverging, with volume increasing rapidly while pressure stays low. This is a classic sign of:
a) Proper intraperitoneal insufflation.
b) Intraluminal insufflation.
c) Preperitoneal insufflation.
d) A large leak or intravascular placement.
-
What is the approximate maximum volume of gas the preperitoneal space can hold at a pressure of 12 mmHg?
a) 200 mL
b) 1 Liter
c) 5 Liters
d) It has unlimited capacity.
-
During a difficult laparoscopic colectomy, the splenic artery is injured, causing major hemorrhage. The surgeon is using aggressive suction. What is the appropriate immediate action regarding the insufflator?
a) Decrease the preset pressure to 8 mmHg.
b) Switch the insufflator to the maximum high-flow emergency mode.
c) Discontinue insufflation and convert to laparotomy.
d) Switch to the pediatric mode to reduce flow.
-
What is the correct way to position a CO2 gas cylinder connected to an insufflator?
a) Horizontally, to ensure stable placement.
b) Upside down, to utilize gravity.
c) Upright or slightly inclined.
d) The position does not matter.
-
Even when using the Hasson (open) technique, it is recommended to start insufflation at a low flow rate (1 L/min) primarily to:
a) Confirm the trocar is not in the preperitoneal space.
b) Prevent a sudden pressure rise that could cause a vasovagal response.
c) Save CO2 gas.
d) Test the patency of the Hasson cannula.
1_B, 2_C, 3_B, 4_B, 5_C, 6_C, 7_D, 8_C, 9_C, 10_C, 11_A, 12_D, 13_B, 14_B, 15_C, 16_B
-
Which of the following pressure settings is most appropriate for a totally extraperitoneal (TEP) inguinal hernia repair?
a) 8 mmHg
b) 12 mmHg
c) 20 mmHg
d) 30 mmHg
-
The "Total Gas Volume" indicator on an insufflator is useful for all the following EXCEPT:
a) Estimating the patient's abdominal capacity.
b) Detecting a large, ongoing gas leak.
c) Differentiating between intraperitoneal and intravascular placement.
d) Measuring the real-time intra-abdominal pressure.
-
In a tall, grand multiparous patient with a very lax abdomen, what is a reasonable expectation for achieving a pneumoperitoneum of 12 mmHg?
a) It will require less than 1.5 L of CO2.
b) The actual pressure will rise to 12 mmHg within the first 500 mL.
c) It may require up to 6 L of CO2.
d) The flow rate will remain at zero throughout.
-
A normal adult patient's abdomen has been successfully insufflated to a pressure of 12 mmHg. The surgeon notices the actual flow rate is consistently 0.5 L/min. This indicates:
a) The patient is in the preperitoneal space.
b) There is a continuous gas leak of 0.5 L/min from a port site.
c) The insufflator is malfunctioning.
d) The CO2 cylinder is nearly empty.
17_C, 18_D, 19_C, 20_B
MOTIVATIONAL MESSAGE FROM DR. R. K. MISHRA:
Your greatest instrument in the operating room is not the scalpel or the laparoscope, but a disciplined mind that remains ever-curious and perpetually vigilant. True mastery is achieved when knowledge becomes instinct and safety becomes reflex.
May your hands remain steady, your judgment sharp, and your dedication to learning endless as you serve your patients. My best wishes are with you.