
A recently published narrative review in Current Opinion in Urology (16 June 2026) highlights an important evolution in surgical education: the transition of nontechnical skills training from subjective observation to structured, measurable, and technology-assisted assessment. Although the review does not present new clinical outcome data, it provides a comprehensive overview of emerging educational strategies that are increasingly relevant to robotic and minimally invasive surgery worldwide.
Traditionally, surgical training has focused heavily on technical competence—tissue handling, dissection, suturing, and procedural execution. However, growing evidence from human-factors research suggests that a substantial proportion of preventable adverse events in the operating room are linked not to technical errors but to failures in communication, teamwork, leadership, situational awareness, and decision-making. As laparoscopic and robotic procedures become more complex, these nontechnical skills have become essential determinants of patient safety and operative success.
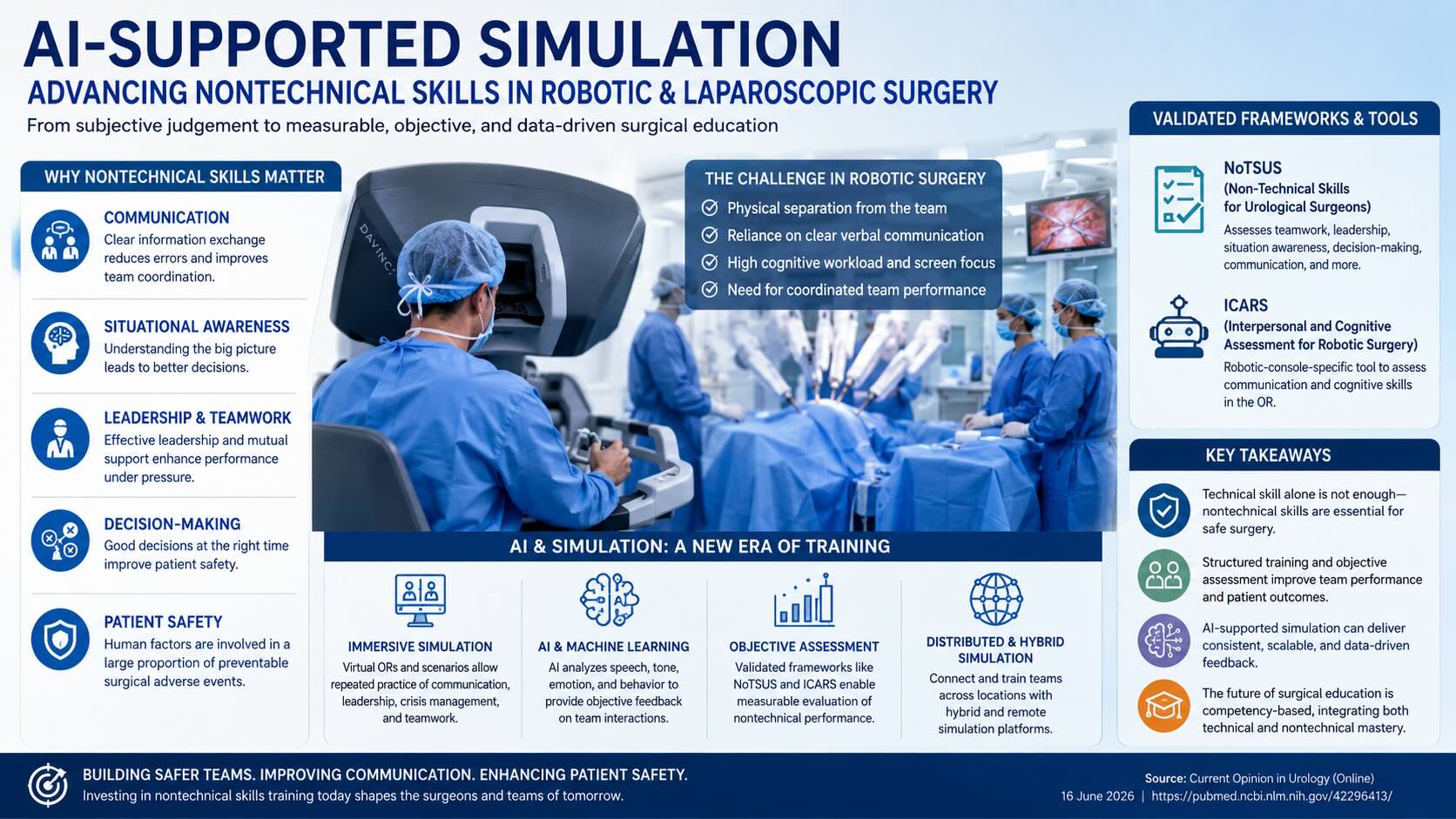
The review discusses several validated assessment systems, including the Non-Technical Skills for Urological Surgeons (NoTSUS) framework and the Interpersonal and Cognitive Assessment for Robotic Surgery (ICARS) model. These tools allow educators to objectively evaluate surgeon behavior in domains such as communication effectiveness, leadership, team coordination, situational awareness, workload management, and decision-making under pressure. By providing standardized scoring systems, these frameworks reduce reliance on subjective faculty impressions and improve consistency in trainee assessment.
One of the most significant developments highlighted is the increasing role of robotic-console-specific communication training. In robotic surgery, the console surgeon is physically separated from the patient and operating team. Unlike open surgery, where verbal and nonverbal cues are readily available, robotic procedures require deliberate and structured communication. Surgeons must effectively coordinate with bedside assistants, scrub nurses, anesthesiologists, and trainees despite physical separation and visual immersion within the robotic console. This unique environment creates opportunities for communication breakdowns that may compromise efficiency and safety if not properly addressed during training.
The review also emphasizes the rapid expansion of simulation-based education. Modern simulation platforms now extend far beyond technical skill rehearsal. Virtual operating rooms, immersive team-training environments, and virtual patient encounters allow surgeons and trainees to practice communication, crisis management, leadership, conflict resolution, and decision-making without exposing patients to risk. These simulation environments can recreate rare but critical events such as unexpected bleeding, equipment malfunction, anesthetic emergencies, or intraoperative complications, enabling teams to develop coordinated responses before encountering such situations in real clinical practice.
An especially promising development is the integration of artificial intelligence, machine learning, and large language models (LLMs) into surgical education. Emerging systems are being designed to analyze verbal interactions during simulated procedures, evaluate communication patterns, detect emotional tone, identify leadership behaviors, and assess team dynamics. AI-powered educational platforms may eventually provide immediate, objective feedback regarding communication quality, situational awareness, and team performance. Such systems could significantly reduce faculty workload while simultaneously increasing the frequency and consistency of trainee assessments.
The concept of distributed and hybrid simulation is another important theme discussed in the review. Traditionally, simulation training required physical attendance at specialized training centers. Advances in digital technology now allow geographically separated learners to participate in collaborative simulations through online platforms. This approach has particular relevance for international fellowship programs, rural surgical training, and continuing medical education, where access to dedicated simulation facilities may be limited.
For laparoscopic and robotic surgery programs, the implications are substantial. Surgical competence can no longer be defined solely by case volume or technical proficiency. A surgeon who performs complex procedures flawlessly from a technical perspective may still pose safety risks if communication, leadership, or situational awareness are inadequate. Modern competency-based education increasingly recognizes that technical and nontechnical skills must develop together.
The review further suggests that future credentialing pathways may incorporate objective measurements of nontechnical performance alongside technical assessments. Just as simulators currently evaluate dexterity and procedural efficiency, future training programs may use AI-assisted systems to certify communication competence, crisis-resource management, and team leadership capabilities before surgeons progress to advanced independent practice.
For institutions involved in advanced laparoscopic and robotic training, these findings support greater investment in structured simulation curricula, faculty development programs, and objective assessment tools. Training centers that integrate technical simulation with human-factors education may be better positioned to produce surgeons capable of delivering safe, efficient, and high-quality minimally invasive care.
Clinical Significance for Laparoscopic Surgeons
As minimally invasive surgery continues to evolve, nontechnical skills should be regarded as core operative competencies rather than supplementary attributes. Communication failures, inadequate situational awareness, and ineffective leadership remain major contributors to preventable surgical errors. AI-supported simulation and objective assessment frameworks offer a pathway toward more reliable training, improved team performance, and enhanced patient safety. The future of laparoscopic and robotic education is likely to be defined not only by how well surgeons operate, but also by how effectively they communicate, lead, and collaborate within increasingly sophisticated surgical environments.
Source: PubMed – Current Opinion in Urology, published online 16 June 2026.