Laparoscopic Hand Instruments, Accessories and Ergonomics
READ ABOUT LAPAROSCOPIC EQUIPMENT AND INSTRUMENTS
Because of the complex modern technology, any things can go wrong. Equipment and instrumentation possess a much greater impact and importance in laparoscopic surgery. This is a proven fact that visualization and tactile exploration of the operative field is definitely only indirectly achieved through optical systems and instruments. The surgeon must be sufficiently acquainted with the equipment to make use of it, troubleshoot and solve the inherent problems.
IMAGING SYSTEM
Imaging system includes the Laparoscope, Light source, Light cable, Camera, and Monitor.
A. Laparoscopes: Laparoscopes are either rigid or fibre optics. Popular are rigid ones, like 0°, 30°, 3mm, 5mm, and 10mm. The 30° angled scopes can be rotated and can see down as well look up the anterior abdominal wall and side ways. The scope is attached with light cable and the distal tip is inspected for fibre bundle transmission. If the fibre damage is 25% or more then the scope must be replaced.
B. Source of light: The brand new source of light for example 250 watt halogen lamp continues to be supplied with a condenser system, But Xenon lamp gives better visual clarity. The light intensity can be regulated manually or automatically. High intensity Xenon lamp gives better visual and photographic clarity.
C. Light Cable: Light carrier is very important. It may either be a fluid or perhaps a glass fibre light cable. Within the cable, there shouldn't be sharp bends and cracks in the plastic sheath, if it's there, then your cable ought to be changed for good light transmission. The cable is available at different diameters and lengths. The diameter of the fibre bundle ought to always be chosen slightly larger then your lens system and should not be too long.
D. Cameras: Now high resolution, small , light weight cameras are available, which is easy to handle, they offer picture of optimal sharpness, high resolution and excellent colour reproduction. Just one chip camera has resolution of point 450-600; But the 3 chip cameras with increased then 750 horizontal lines give excellent visual clarity. Usually single chip camera is adequate for routine laparoscopic surgeries but when surgery is recorded for later inclusion in larger film or video production, three chip camera is preferable. Now a recent version of digital 3 chip camaras with integrated image processing modules can be obtained.
E. Monitors: The video monitor must generate high res image after the S-VHS connection. Larger video screen is preferred, 20 inches and above, non flickering medical monitors rich in resolutions more then camera is preferred.
Gas for pneumoperitonium
Air was the first gas used to produce pneumoperitoneum, but has largely been abandoned. The primary drawback to air may be the risk of air embolism.
Characteristics from the ideal insufflating agent
- The ideal insufflating agent during laparoscopic procedures should be colorless, physiologically inert, and non explosive in the presence of electrocautery or laser coagulation.
- Its solubility in blood should be high.
- The insufflating gas ought to be readily available, inexpensive, and nontoxic.
1. Co2: Co2 is an odorless, colorless gas. It's a easily available, stable, naturally formed within the tissues and subsequently eliminated by the lungs. Due to these functions, Co2 is easily the most commonly used gas for insufflation during laparoscopic procedure.
Advantages
- It has relatively safe of venous gas embolism
- It doesn't support combustion
Disadvantages:
- Hypercarbia and acidosis
- The direct effects of carbon dioxide and acidosis canlead to decreased cardiac contractility, pulmonary hypertension and systemic vasodilation.
- Nitrous Oxide
Nitrogen is biologically inert, colorless, gaseous element that is found free in the air. Nitrous oxide has been suggested for that procedures performed under local anesthesia, or for patients with pulmonary disease undergoing longer procedures.
Advantages
- Insignificant alterations in acid-base balance.
- Decreased pain
Disadvantages
- Supports combustion in the presence of hydrogen or methane gas.
- Helium (He)
Helium is a colorless, odorless, tasteless gas that's from gas. This inert gas is neither combustible itself, nor supports combustion. Helium is less soluble in water than co2.
Advantage:
- The main physiologic advantage may be the minimal effect on acid- base balance.
Disadvantages
- The development of postoperative subcutaneous emphysema continues to be observed, because it is relatively poorly soluble in water.
- Risk of venous gas embolism since it is less soluble in water then carbon dioxide. It is more diffusible because of its low density.
4. Argon
Argon gas is colorless, odorless, noncombustible, and chemically nonreactive.
Advantage
- The major physiologic advantage is stable acid base status.
Disadvantage
- The major possible physiologic disadvantage is cardiac depression.
LAPROFLATTOR
The Electronic CO2 Laproflattor is really a general purpose insufflation unit to be used in laparoscopic operations. Controlled pressure insufflation of the peritoneal cavity can be used to achieve the necessary work area for laparoscopic surgery by distending the abdominal wall and depressing the hollow organs. Automatic insufflators allow the surgeon to preset the insufflating pressure also it supplies gas until the required intra-abdominal pressure is reached. The insufflator activates and delivers gas automatically when the intra-abdominal pressure falls due to gas escape or leakage from the ports. Insufflation pressure could be continuously varied from 0 to 30 mm Hg; total gas flow volumes can be set to any value in the range 0-9.9 liters/mm. Patient safety factors are ensured by optical and acoustic alarms in addition to several mutually independent safety circuits. The important indicators of insufflators are preset pressure, actual pressure, flow rate and total gas used.
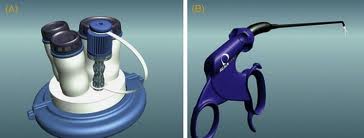
Suction Irrigation Machine
It is employed for flushing the abdominal cavity and cleaning during endoscopic operative intrusions. It's been designed for use with the 26173 AR suction /instillation tube. Its electrically driven pressure/suction pump is protected against entry of bodily secretions. The suction irrigation machine can be used frequently during the time of laparoscopy to create the concept of vision clear. Most of the surgeons use normal saline or ringer lactate for irrigation purposes. Sometimes, heparinized saline can be used to dissolve blood clot to facilitate proper suction in the event of excessive intra-abdominal bleeding. Suction and Irrigation hand apparatus. Irrigation and suction are necessary during laparoscopic surgeries specially to maintain clear visual field and maintained hemostasis. It comes in 5mm and 10mm reusable sizes. The suction tip is extremely helpful for intermittent suction and as blunt dissecting instrument in place of finger, as we use within conventional surgeries.
Operative hand instruments
Reusable and disposable instruments are commercially accessible. Disposable instruments provide better performance and better safety on single use. To make it cost effective the surgeon has to reuse the disposable instruments after sterilisation. Reusable instruments are significantly cheaper in the long run, however, they require proper cleaning and maintenance.
Veress Needle
Veress needle was introduced by a chest physician for aspiration of pleural effusion keeping in mind that it is spring mechanism and blunt tip may prevent the injury of lung tissue. Veress needle includes an outer cannula with a beveled needle point for cutting through tissues ((blank) 8). Inside the cannula it comes with an inner stylet, which is packed with a spring. This spring springs forward in response towards the sudden decrease in pressure encountered upon crossing the abdominal wall and entering the peritoneal cavity. The lateral hole about this stylet enables CO2 gas to become delivered intra-abdominaly. Veress needle is used for creating initial pneumoperitoneum so the trocar can enter safely and also the distance of abdominal wall from the abdominal viscera should increase. Veress needle way is probably the most widely practiced way of access. It is crucial to check veress needle each time before using it, for its (1) potency and, (2) spring action. Veress needle will come in three lengths 80mm, 100mm and 120mm. In obese patient 120mm and in very thin patient with scaphoid abdomen 80mm veress needle ought to be used. Veress needle should be held like a dart at the time of insertion.
2. Hassan Cannula
It's less commonly used than veress. It usually cuts down on the risk of vascular and hollow visceral injury. It's an extremely safe instrument to go in the abdomen, particularly in a patient that has previously undergone intra-abdominal procedures. This cannula consists of three pieces: a cone-shaped sleeve, a metal or plastic sheath with a trumpet or flap valve, along with a blunt tipped obturator. About the sheath there are two struts for affixing two fascial sutures. These sutures are then wrapped tightly around the struts. Thereby firmly seating the cone shaped sleeve into the laparoscopic port. This creates a highly effective seal to maintain penumoperitoneum.
B. Trocars
The term “trocar” is usually used to refer to the whole assembly but actual trocar is a stylet that is introduced with the cannula. The trocars are available with different type of tips. The cutting tips of those trocars are generally in the shape of a 3 edged pyramid or a flat two edged blade. Conical tipped trocars are meant to be less traumatic towards the tissue. The tip can be penetrated through the parietal wall without cutting along with a decreased risk of herniation or haemorrhage is reported.
Cannulas have been in general produced from plastic or metal. Plastic devices whether they are transparent or opaque, need to be designed in such a way as to minimize the reflection of light from the telescope. Reusable and disposable trocars are constructed by a mixture of metal and plastic. The tip of disposable trocar includes a two edged blade. These are extremely effective at penetrating the abdominal wall by cutting the tissue as they pass through. Most of the disposable plastic trocar has a spring loaded mechanism that withdraws the sharp tip immediately after it passes through the abdominal wall to reduce the incidence of injury of viscera. Trocar and cannula are of various sizes and diameter depending upon the instrument that it is used. The diameter of cannula ranges from 3 mm to 30 mm; the most typical size is 5mm and 10 mm. Newer and more effective disposable trocar designs incorporate unique design features such as direct serial incision from the tissue under visual control.
All of the cannulas have a valve mechanism at the very top. Always inspect the trocar to ensure that all the valves move smoothly and, that the insufflation valve is closed (to prevent losing pneumoperitoneum). The valves of cannula provide internal air seals, which permit instruments to move in and out within cannula with no loss of pneumoperitoneum. These valves can be oblique, transverse, or perhaps in piston configuration. These valves can be manually or automatically retractable during instrument passage. Surgeon should remember that sharp trocars although looking dangerous are actually better than blunt ones, because they need less force to introduce inside the abdominal cavity and the likelihood of inadvertent forceful entry of full length of trocar is lesser. The finish from the cannula is either straight or oblique. An oblique tip is felt to facilitate the simple passage from the trocar through the abdominal wall.
C. Reducing Sleeve: It's used to reduce the size of the main harbour from 10mm to 5mm or 5mm to three mm, to ensure that pneumoperitoneum is maintained when ever surgeon changes the instrument from larger diameter to smaller diameter.
D. Needle holder: Laparoscopic needle holder can be obtained with a straight or curved tip. Two needle holders are essential to perform swift endo-suturing, although endo-suturing can be done satisfactorily with a single needle holder along with a grasper. In-line grip needle holders are ergonomically much better than pistol grip needle holder.
E. Port closure instrument: They are self innovative hand instruments to close the laparoscopic ports, especially 10mm or larger ports, as needed
Disposable or Reusable Instruments
Several factors should be considered during the time of choosing laparoscopic instrument, including cost, availability and reliability. Reusable instruments are costly initially but in long run they are economical. In developing countries, disposable instruments are very rarely used because labour price is low compare to the cost of disposable instrument. In Europe and USA, surgeons often choose to use disposable instrument to save high labour cost. The disposable instruments aren't sterilized properly by dipping in gluteraldehyde because they are not dismountable. Insulation of disposable instrument also can be torn easily be responsible for electrosurgical injuries.
Laparoscopic hand instruments vary in diameter from 1.8 to 12mm but majority of instruments are made to go through 5 to 10mm of cannula. The instruments will also be of various lengths (vary from company to company, usually varies from 18 to 45cm) but you are ergonomically convenient to use if they have same length of approximately 36 cm in adult and 28 cm in pediatric practice. Shorter instruments 18 to 25cm are adapted for cervical and pediatric surgery. Certain procedures for adult can also be performed with shorter instrument in which the space is constricted. Forty-five centimeter instruments are utilized in obese or very tall patients. For better ergonomics 1 / 2 of the instruments should be inside the abdomen and half outside. If half of the instrument is in and half out, it behaves like a class-1 lever; and it stabilizes the port nicely and thus surgery becomes convenient. Most of the laparoscopic procedures need a mixture of sharp and blunt dissection techniques, often utilizing the same instrument in a number of different ways. Many laparoscopic instruments can be found in both re-usable and disposable version. Most re-usable instruments are partially dismountable in order that it can be cleaned and washed properly. Some manufacturer have produced modular system where the main instrument could be changed to suit the surgeon favorite attachment like handle or working tip.
Most laparoscopic instruments like graspers and scissors have basic opening and closing function. Many instruments manufactured during past few years can rotate at All over angle which boosts the degree of freedom of these instruments.
Most of the hand instruments have three detachable parts.
a) Handle
b) Insulated outer tube
c) Insert which makes the end from the instrument.
Certain instrument handles are made to allow locking of the jaw. This is very useful when the tissue must be grasped firmly for long period of time preventing the surgeons hand from getting fatigued. The secure is usually incorporated into the handle so that surgeon can certainly lock or release the jaws. Scalping strategies will often have a ratchet so the jaws could be closed in various positions and to different pressures. The majority of the laparoscopic instrument handles have attachments for unipolar electrosurgical lead and many have rotator mechanism to rotate the tip of the instrument. Some multifunctional laparoscopic handles have attachment for suction and irrigation. The Cuschieri Ball Handle was introduced by Prof. Sir Alfred Cuschieri. This handle lies comfortably in surgeon’s palm. This design reduces the fatigue of surgeon and eases rotation of the instrument by getting rotation inside the palm instead of using wrist rotation. Squeezing the leading from the handle between your thumb and the first fingers increases the jaw closing force; squeezing the trunk from the handle between your thenar eminence of the thumb and last fingers opens the jaws. Cuschieri pencil handle also offers great ergonomic value specially when combined with needle holder. This handle allows the angle between your handle and the instrument to be altered to suit the surgeon’s wrist angle. The conveniently placed lever of the pencil handle when pressed can change the angle. Just like ball handle, pressure in front boosts the jaw closing force while pressure at the rear opens the jaw. Insert of hand instrument varies only at the tip. It may be grasper, scissors, or forceps. This grasper may have single action jaw or double action jaw. Single action jaw open under double action jaw but close with greater force thus, the majority of the needle holders are single action jaw. The necessary wider opening in double action jaw exists in grasper and dissecting forceps. Single action graspers and dissectors are utilized where more force is needed.
D. Different kind of Graspers
These graspers are good when you don’t have total control over depth and surgeon really wants to are employed in single plane in controlled manner particularly during adhesiolysis.
E. Instruments for Sharp Dissection
- Scissors
- Electro surgery hook
- HF Electro surgery spatula (Berci)
- HF Electro surgery knife
- Knife
Scissors are one of the oldest surgical instruments used by surgeons. Scissors are utilized to perform many tasks in open surgical treatment but its use in minimal access surgery is restricted. In minimal access surgery scissors require greater skill because in inexperienced hand you can get unnecessary bleeding and damage to important structures
- Kinds of Laparoscopic Scissors
- Straight Scissors
- Curved Scissors
- Serrated Scissors
- Hook Scissors
- Micro-tip Scissors
Spatula, Hook and Harmonic Scalpel
Spatula has a flat tip for dissecting the gallbladder in the liver bed. It is much safer than the hook. Hook has a L shaped tip. Usually it is accustomed to dissect the gallbladder from the bed of the liver. Some surgeons also use this instrument for opening of the intestine. Now a days in modern laparoscopic surgery ultrasonic scalpel (Harmonic scalpel) can be obtained for advanced procedures. They are available as either disposable or reusable. Reusables are of of three sizes, large, medium large and medium. They are used to clip cystic artery and cystic duct based on their size. Disposable clip applier includes preloaded 20 clips per unit since the Protack (popular in mesh repair in hernia) is available in 30 per unit.
ERGONOMICS
- Word derivation: ergon and nomia
- Concept: of designing the working environment to fit the worker, rather than forcing the worker to fit the significant environment
- Application: to make the OT more user-friendly, to reduce stress, to increase efficiency and safety
- Includes: instrument, machines and OT design
- Involves: understanding the interactions between humans along with other elements within the system to optimize human well-being and overall performance from the system
Operative laparoscopy has changed the concept of surgery from prolonged painful recuperative periods with long scars of open surgery to short stay, painless, and cosmetically satisfying surgery. It's been achieved at the expense of surgeons’ discomfort and fatigue, thus putting both surgeon and patient in danger. Inadequate understanding of ergonomics together with ergonomically deficient design of laparoscopic instruments has been cited as you possibly can causes. Increased technological complexity and sometimes poorly adapted equipment have resulted in increased complaints of surgeons’ fatigue and discomfort during laparoscopic surgery.
Ergonomic Variable
The important variables that have been studied include hand size, handle to tip force transmission, optimum height from the surgeon’s hand and height of the operating table, view site with regards to monitor position and the technique of gripping the instruments.
Hand size
Hand size is an essential variable to consider when designing laparoscopic hand tools. This is because laparoscopic surgeons, especially women using glove sizes 6.5 or smaller, experience musculoskeletal problems while using the common laparoscopic instruments. Moreover, subjects who reported musculoskeletal problems performed a significantly greater percentage of laparoscopic cases and located the stapler and graspers difficult to use for any greater percentage of time than those not reporting problems.
Handle to tip force transmission
Data in the Society of yankee Gastrointestinal and Endoscopic Surgeons (SAGES) reveal that laparoscopic instruments are afflicted by ergonomically inadequate handle designs and inefficient handle to tip force transmission, which lead to surgeons’ fatigue, discomfort, and hand paresthesias. Studies quantifying forearm and thumb muscle workload by processed electro-myogram (EMG) demonstrated that the peak and total muscle effort of forearm and thumb muscles were significantly greater when the grasping task was performed using the laparoscopic instrument. It was discovered to be more prevalent among junior laparoscopic surgeons having under 2 yrs of experience.
Optimum height
Discomfort and difficulty ratings were lowest when instrument handles were positioned at elbow height. The positioning of laparoscopic instrument handles needed to be near to surgeons’ elbow level to minimize discomfort and upper arm and shoulder muscle work. It was found to match an approximate table height of 64 to 77 cm above floor level.
Technique of gripping
Palm grip hand position using the pistol handle (thumb away from ring with the palm resting about the thumb ring) is more efficient than the finger-in-ring grasp since it significantly reduces the muscle forces required for grasping having a laparoscopic instrument. Many surgeons do, in fact, use the palm grasping hand position for sustained grasping tasks during laparoscopic surgery. Moreover, use of finger tips rather than finger base during finger-in-ring grasp during tissue dissection reduces discomfort. Most of the surgeons performing regular laparoscopy are not aware the complications of nerve injury and neuropraxia following improper gripping technique. Experience in laparoscopic surgery does play a major effect on knowledge about ergonomical problems. Operating for prolonged hours with eyes focused on video monitors results in eye strains among laparoscopic surgeons. Placement and adjustment of monitors have little benefit in improving the situation though experience led to some improvement. Utilization of laparoscopy is associated with significant ergonomic problems, hence proper training and awareness among laparoscopic surgeons is essential in India. This is only possible if an authorized accreditation council sets up guidelines and oversees working out programs, thus making laparoscopy safer for both surgeons and patients.
Recommended Laparoscopic Instruments for Surgeons:
